



Research on NiTi instruments combined with ultrasonic irrigation and multiantibiotic paste in root canal therapy of periapical inflammation in deciduous teeth
- Authors:
- Published online on: July 3, 2024 https://doi.org/10.3892/etm.2024.12635
- Article Number: 346
-
Copyright: © Zhu et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
Introduction
In periapical lesions of deciduous teeth, the apex and bifurcation sites, encompassing the cementum, periodontal ligaments and alveolar bone, can harbor co-infections involving anaerobic bacteria and other pathogens (1). These infections may trigger heightened osteoclast activity or alveolar bone resorption (2). In severe cases, infection may extend to permanent teeth, precipitating premature loss of primary teeth and adversely affecting the typical growth and development of permanent teeth (3,4). Root canal treatment is the foremost intervention for periapical disease in deciduous teeth. This treatment not only proves effective in alleviating pain, controlling inflammation and encouraging lesion healing, but also supports the natural turnover of deciduous teeth, thereby preserving the typical development of permanent teeth (5,6). The success of root canal treatment relies on the effective control of bacterial infections within the root canal, a pivotal step encompassing the removal of infectious material, root canal disinfection and subsequent filling with absorbable materials (7,8). Presently, the manual use of stainless steel files remains the primary instrument for root canal treatment in pediatric deciduous teeth (9). Nevertheless, a previous study reported that NiTi root canal preparation devices exhibit promise for treating infections in deciduous teeth, particularly in the mechanical preparation step (10). Additionally, optimizing root canal lengths has proven instrumental in enhancing the efficiency and safety of root canal preparation, thereby substantially reducing bacterial counts and metabolites within the root canal (11,12). The practice of enlarging the root canal preparation area has gained traction in clinical practice, demonstrating its capability to mitigate postoperative responses and achieve heightened postoperative filling rates (13). However, the intricate anatomy of the root canal may pose challenges to accomplishing the desired resection through mechanical preparation with a NiTi instrument.
Antibiotics serve a crucial role in the clinical control of root canal infections and are a valuable complement to mechanical cleaning (14). While effective mechanical cleaning coupled with antibiotic sealing holds the potential for superior root canal disinfection, this combination has not been extensively reported. Nakamura et al (15) reported that antibiotics, in conjunction with ultrasonic flushing, were more effective than nonactivated irrigation in enhancing root canal cleaning. However, Klyn et al (16) reported that there was no significant difference in the cleaning efficacy when antibiotics were combined with ultrasonic flushing or other debridement methods in the apical region. Therefore, after the ultrasonic treatment (with or without NiTi device), the removal of infectious substances and microorganisms using appropriate intracanal medications or rinses is a pivotal step in the treatment process for root canal infection.
Given the diverse range of microorganisms that can infect root canals, relying on a single antimicrobial drug may fall short in achieving thorough disinfection. Therefore, tailored antibiotic use combining multiple drugs into a paste, based on the common flora identified in root canal lesions, may effectively control inflammation and inhibit bacterial proliferation (17). Cogulu et al (18) reported that pathogenic bacteria in children with periapical lesions are predominantly anaerobic, often mixed with other bacteria like Clostridium sclerotinia and Streptococcus. Clinical manifestations of these infections include pain, discomfort upon percussion, root canal exudate and pus formation (19). A commonly used antibiotic combination for the treatment of these pathogens is the metronidazole, ciprofloxacin and minocycline paste (20). This paste, composed of the aforementioned antibiotics, not only exhibits broad-spectrum antibacterial properties, but also demonstrates robust efficacy, rendering it widely applied in clinical practice.
Cefixime, a third-generation cephalosporin antibiotic, demonstrates high stability against β-lactamase produced by gram-negative bacilli and exhibits potent bacteriostatic activity (21). Its efficacy against gram-negative bacilli in the oral cavity surpasses that of both first- and second-generation cephalosporins, making it highly suitable for treating root canal infections (22). By contrast, dexamethasone is an adrenocorticosteroid drug renowned for its anti-inflammatory, anti-allergic and analgesic effects and is therefore used to reduce pain in root canal treatments (23,24).
The present study aimed to assess the clinical efficacy of a mechanical NiTi file combined with ultrasonic cleaning and multiple antibiotic paste through a randomized controlled study. The incorporation of cefixime and dexamethasone, alongside additional antibiotics, into an existing triple antibiotic regimen will deepen understanding of treating periapical inflammation in deciduous teeth. This study aimed to provide further knowledge and practical guidance for enhancing treatment outcomes and the overall quality of life for patients undergoing root canal treatment.
Materials and methods
Clinical data collection
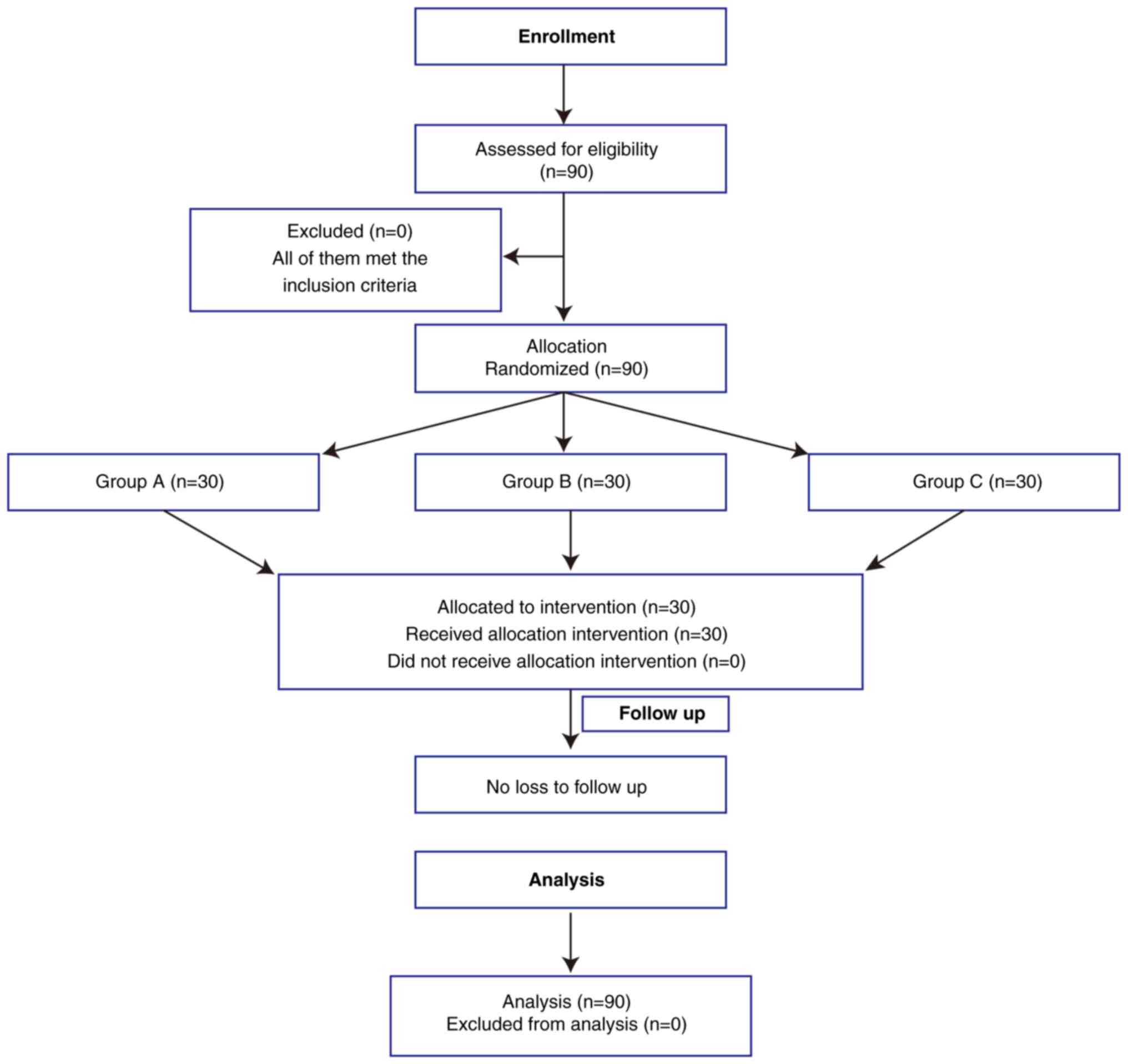
The present study received approval from the Medical Ethics Committee of the Affiliated Hospital of Southwest Medical University (approval no. 20200916002; Sichuan, China). The recruitment of subjects commenced in October 2020 and concluded in October 2021. All participants were enrolled from the Department of Pediatric Stomatology at The Affiliated Stomatological Hospital of Southwest Medical University (Sichuan, China). A total of 90 patients, each with one tooth exhibiting periapical inflammation, were selected as the subjects for the study. During the course of the study, the legal guardian of all children provided written consent for participation in the study.
Study design and inclusion and exclusion criteria
A total of 90 patients were randomly assigned to groups A, B and C (n=30/group), in the process of root canal preparation. The inclusion of two control groups (B and C) was designed to compare the efficacy of the intervention. Both group A and group B were prepared by using M3 primary tooth machine and nickel-titanium file. In group A, ultrasonic root canal washing was combined with multiple antibiotics sealing (metronidazole, ciprofloxacin, minocycline, cefixime and dexamethasone) followed by two weeks of root canal filling. In group B, ultrasonic root canal washing was performed followed by calcium hydroxide sealing for two weeks. In group C, root canal was prepared using stainless steel hand K-file followed by calcium hydroxide sealing for two weeks of root canal filling. By having two control groups, the relative efficacy of the proposed intervention in comparison to different treatment strategies could be assessed. This design allowed for a more comprehensive evaluation of the intervention's efficacy in the context of treating periapical inflammation in deciduous teeth.
The inclusion criteria for the study were as follows: i) A definitive diagnosis of acute or chronic periapical inflammation of deciduous teeth; ii) the affected root was in a stable stage (patient aged 4-7 years) which is the period of time from the formation of deciduous tooth roots to their resorption and X-ray images demonstrate no root atresia calcification or root resorption; iii) The FrankI treatment compliance evaluation scale was utilized to score the degree of compatibility and all scores were >3 points (25); and iv) informed consent was provided by the patient's legal guardian.
The exclusion criteria for the study were as follows: i) History of antibiotic therapy within the last 1 month; ii) history of antibiotic allergies; iii) contraindications to root canal treatment; iv) pulp penetration and root divergence; v) patients who did not cooperate with treatment and exhibited poor compliance; vi) incomplete medical records; and vii) patients with systemic diseases.
Experimental materials
A multi-antibiotic paste, composed of metronidazole (0.2 g/tablet, Huazhong Pharmaceutical Co., Ltd.; approval no. H42020388), ciprofloxacin (0.25 g/ capsule; Zhejiang Jingxin Pharmaceutical Co., Ltd.; approval no. H33020387), minocycline (0.1 g/capsule; Hanhui Pharmaceutical Co., Ltd.; approval no. H20174081), cefixime (0.1 g/capsule; Chengdu Brilliant Pharmaceutical Co., Ltd.; approval no. H20041661) and dexamethasone (0.75 mg/tablet; Guangdong Nanguo Pharmaceutical Co., Ltd.; approval no. H44024618) was prepared in equal proportions at a ratio of 1:1:1:1:1.
Intervention
All patients underwent X-ray imaging prior to root canal treatment. Patients underwent initial, secondary, tertiary and follow-up visits during the treatment regime.
Initial visit
Patient diagnosis and treatment planning were carried out and newly diagnosed cases underwent the removal of caries, pulp opening and hole preparation. The top of the pulp chamber was removed, and the pulp was extracted. The affected area was rinsed, and moisture was removed by drying the area. The area was sealed with calcium hydroxide (Ivoclar Vivadent ApexCal; approval no. 20153172564) for 1 week.
Second visit. The sealing agent was removed, and the root canal extracted using a 15K file (Dentsply Sirona) lubricated with 17% EDTA (Longly Biotechnology). Root ZX root canal measuring instrument was used to measure the root canal length of group A and group B. Root canal preparation was performed with the M3 baby tooth file combined with ultrasonic cleaning (Yirui M3 taper 0.06; Changzhou Yirui Machinery Processing Co., Ltd.) In Group C, root canals were enlarged with a Gates Glidden drill (Dentsply Sirona) and prepared by hand with stainless steel K files (Dentsply Sirona; nos. 15, 20, 25 and 30) in combination with 17% EDTA. The root canal was rinsed with ≥5 ml of a 0.25% sodium hypochlorite solution and flushed with 0.9% normal saline. In Group A, the tip of the root canal was dried using hygroscopic paper and was subsequently filled with the multiple antibiotic paste before being temporarily sealed using glass ionomer (Changshu Shangchi Dental Materials Co., Ltd.; approval no. 20193171718). In Groups B and C, the root canal was dried with tissue, filled with 23.9% ApexCal Calcium hydroxide and temporarily sealed with glass ionomer.
Third visit. Patients returned 2 weeks after drug sealing and if there were no obvious issues and the local mucosa returned to its normal state, the paste in the root canal was washed away with purified water. The root canal lumen with filled with vitex paste (Neo Dental Chemical Products Co., Ltd.), a material based on glass ionomer cement, and filled with composite resin. If there were no obvious issues 1 week after filling, a pre-coronation examination, which includes oral examination and X-rays, was performed to ensure the effectiveness of root canal treatment and the stability of the filling. Root canal treatment was performed by the same doctor.
Follow-up visits. Follow-up visits were conducted at 6 and 12 months after root canal treatment. Clinical symptoms of the affected tooth and the condition around the root were recorded by X-ray. X-ray records were completed by the dental assistant.
Evaluation of pain intensity
Following the surgery, the pain level of patients was assessed through a questionnaire analyzing pain scores. A WeChat (Tencent; version 8.0.40) mini-program facilitated pain follow-ups on 1, 3 and 7 days after the treatment. The Visual Analog Scale (VAS) was employed to gauge the severity of pain among the treatment groups. The scale comprised a total score of 10 points, where higher scores indicated more intense pain. Pain levels were categorized as follows: i) 0 (no pain); ii) 1-3 (mild pain); iii) 4-6 (moderate pain); and iv) 7-10 (severe pain).
Therapeutic efficacy evaluation
The assessment of root canal treatment outcomes was conducted at the 6 and 12-month post-treatment marks, based on a number of criteria. The criteria for an effective treatment were as follows: i) No noticeable loosening or swelling of the treated tooth post-surgery; ii) healing of the original gum leakage; iii) X-rays demonstrated either the disappearance or reduction of shadows in the affected area; and iv) no anomalies in the inherited permanent tooth germs. The criteria for an ineffective treatment were as follows: i) Presence of postoperative bleeding, spontaneous pain, occlusal pain, redness, swelling, sinus formation or tooth loosening; and ii) X-rays demonstrated no substantial changes, an increase in shadows in the thinning area of the apical bone or progressive pathological resorption.
Statistical analysis
Data sorting and analysis were conducted using SPSS software (version 23.0; IBM Corp.). The VAS scores were presented as median ± interquartile range and were analyzed using the Kruskal-Wallis test followed by Dunn's post hoc test. Fisher's exact test followed by Bonferroni's correction was used to analyze the therapeutic effect after root canal treatment. Count data were expressed as percentages.
Results
Study criteria
A total of 90 patients were enrolled in the present study, each having one affected tooth with periapical periodontitis of deciduous teeth (Fig. 1).
Evaluation of pain severity on days 1, 3 and 7 post-treatment
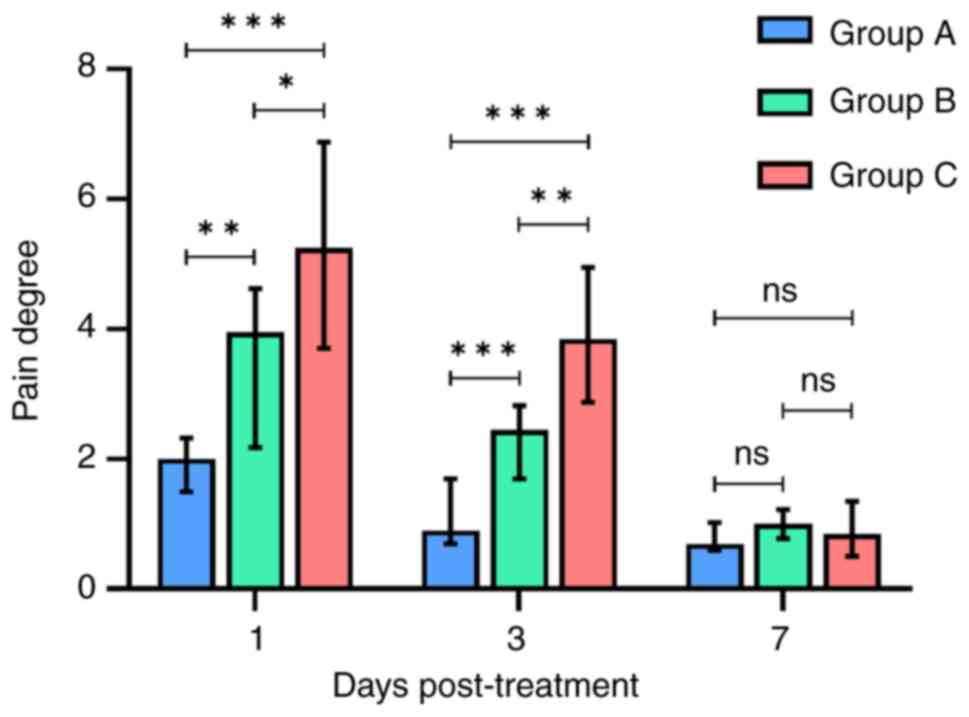
The pain response scores at 1, 3 and 7 days after surgery were analyzed (Fig. 2; Tables SI, SII and SIII). Notably, Group A exhibited significantly lower pain scores compared with Groups B and C on days 1 and 3 post-treatment (P<0.05). Group B demonstrated a significantly lower postoperative pain scores compared with Group C on days 1 and 3 post-treatment (P<0.05). However, by day 7 post-treatment, there was no significant difference in pain scores among the three treatment groups (P>0.05). These findings suggest that, during the early postoperative period, the combined approach of the NiTi device, ultrasonic irrigation and multiple antibiotic treatment administered to Group A may have contributed to superior pain reduction compared with the other treatments.
Evaluation of treatment efficacy at 6 and 12 months post-treatment
The efficacy of the treatments were evaluated 6 months after surgery. X-rays from Group B were used as examples for efficacy evaluation. No abnormal images were detected of the root and germ of the permanent tooth of the left lower second deciduous molar, which indicated effective treatment 6 months following surgical treatment (Fig. 3). Conversely, the distal root resorption of the right lower primary molar displayed a low periapical density shadow, thus was recorded as an ineffective treatment (Fig. 4). The observation of treatment outcomes at 6 and 12 months post-treatment reinforced the distinctions demonstrated between the various treatments applied in the present study. Imaging of the effectively treated teeth exhibited normalcy in the periapical region, whereas ineffectively treated teeth demonstrated significant abnormal shadows. These results highlighted the role of research in assessing therapeutic effects in clinical applications and may offer practical insights for the long-term management of periapical inflammation of deciduous teeth.


At 6 months after the root canal procedures, there was one ineffective case in Group A, two in Group B and eight in Group C, which resulted in an effective treatment rate of 96.66, 93.33 and 73.33%, respectively (Table I). The effective treatment rate in both Groups A and B were significantly higher compared with that of Group C (P<0.05). However, there was no significant difference in the effective treatment rate between Groups A and B (P>0.05). This highlighted the potential superior efficacy observed in Groups A and B compared with Group C at the 6-month interval post-root canal treatment.
In the extended observation at 12 months following root canal treatment, each of the three treatment groups exhibited cases of ineffective treatment (Table II). The effective treatment rate for Group A was 93.33%, which was significantly higher compared with that of Group C which was 63.33% (P<0.05). However, there was no significant difference in the effective treatment rate of Group B (70.00%) and Group C. Neither between Group B and Group A. These findings emphasized the increased efficacy exhibited by the treatment administered to Group A, which suggests its superiority over the treatment administered to Group C over a 12-month period. These data provided support for the efficacy of the treatment protocol implemented in Group A.
Discussion
Root canal treatment stands as a pivotal therapeutic approach in managing apical infections of deciduous teeth, with the overarching objective of facilitating the physiological shedding of deciduous teeth (26). The pivotal role of microorganisms within the root canal system in initiating and perpetuating pulp and periapical ailments underscores the criticality of effectively eliminating bacteria from the root canal for the success of the treatment (27). The intricate anatomy of the root canal, coupled with the deep infiltration of bacteria and debris into dentin tubules, pose challenges to traditional treatment methods such as mechanical NiTi preparation and ultrasonic flushing, particularly in addressing collateral branches of the root canal (28,29). Consequently, the present study employed a randomized controlled design to assess the clinical efficacy of combining mechanical NiTi file preparation with ultrasonic cleaning, alongside the application of a multiple antibiotic paste. This multifaceted approach aimed to overcome the limitations of traditional techniques and enhance the overall efficacy of root canal treatment in deciduous teeth.
The results of the present study demonstrated differences in the pain scores reported among the three treatment groups on days 1 and 3 post-treatment. Specifically, Group A exhibited significantly lower pain VAS scores compared with Groups B and C, with Group B also demonstrating lower scores compared with Group C. By day 7, all treatment groups demonstrated a substantial improvement in pain levels. Post-root canal preparation, pain can stem from inadequacies in the procedure, for example, mechanical injury caused by instrumentations (hand files or rotary) or chemical damages due to disinfection (30). In the present study, the superior pain outcomes in Groups A and B, compared with Group C, suggested that a meticulous approach to root canal preparation and more effective cleaning methods may have contributed to reduced pain levels. The antibiotic pastes employed in the present study displayed efficacy in eradicating Streptococcus and Fusobacterium sclerotia, thereby mitigating swelling, alleviating pain and sterilizing the area. Moreover, the application of glucocorticoids, specifically dexamethasone, exerted inhibitory effects on the inflammatory process, minimizing early inflammatory symptoms such as redness, swelling, heat and pain. The amalgamation of these factors significantly alleviated postoperative pain in Group A compared with Group C. These results suggested that the combined utilization of NiTi mechanical preparations, ultrasonic irrigation and multi-faceted antibiotic therapy presented substantial advantages in reducing pain post-root canal treatment in deciduous teeth. This multifaceted approach potentially holds promise in enhancing the treatment compliance of pediatric patients.
The outcomes of the present study demonstrated notable differences in the effective treatment rates between Group A and Group B. At the 6-month mark post-root canal treatment, coupled with the application of tightly closed metal preformed crowns, Group A and Group B exhibited effective rates of 96.66 and 93.33%, respectively. Effective treatment rates showed a significant disparity at the 12-month mark, with effective rates of 93.33 and 70.00% for Groups A and B, respectively. The superior response rate in Group A compared with Group B could potentially be attributed to the multi-antibiotic treatment administered within 2 weeks after root canal preparation. This intervention served a crucial role in controlling the microorganisms within the root canal, thereby facilitating the recovery of inflammation in the periapical tissue. These findings highlighted the efficacy of the antibiotic regimen administered to Group A, substantiating its role in promoting the resolution of periapical inflammation.
In the present study, the multi-antibiotic protocol adopted in Group A comprised metronidazole, ciprofloxacin, minocycline, cefixime and dexamethasone. Each component in this regimen served a specific purpose to collectively enhance the therapeutic outcome. Metronidazole, classified as a nitroimidazole organic compound, exhibits a broad-spectrum antibacterial effect, particularly against anaerobic bacteria (31). Ciprofloxacin, a fluoroquinolone, exerts potent antimicrobial activity against gram-negative bacteria by primarily inhibiting DNA replication (32). Minocycline, belonging to the tetracycline class, disrupts bacterial protein synthesis, contributing to its antimicrobial effects (33). Cefixime, a cephalosporin antibiotic, demonstrates robust antibacterial efficacy against streptococcal sclerotinia and Fusobacterium (21). Lastly, dexamethasone, a glucocorticoid, possesses anti-inflammatory, anti-allergic and analgesic properties (24).
By contrast, the application of calcium hydroxide as a sealant in Group B, while biologically active and capable of disrupting bacterial biofilms, creating an alkaline environment and neutralizing acidic substances, exhibits antibacterial efficacy inferior to that of certain types of antibiotic pastes (34). Consequently, Group A demonstrated a superior treatment outcome, which was potentially due to the potent antimicrobial properties of its multi-antibiotic regimen. Additionally, the treatment efficiency of Group B surpassed that of Group C. This result may be attributed to the combined use of NiTi mechanical preparation and ultrasonic irrigation, which could facilitate the effective removal of infectious materials and smear layers within the root canal (14). This synergistic approach enhanced the overall treatment efficiency, potentially highlighting the importance of employing multiple treatment strategies for optimal therapeutic results.
Further research should focus on proposing potential mechanisms for the observed effects reported in the present study. Furthermore, a more detailed discussion of limitations, along with suggestions for future research to address these limitations, is encouraged. For example, the use of a single antibiotic compared with the use of mixed antibiotics in the present study to optimize the ratio of the components of the antibiotics mixture. While the findings of the present study may have scientific and clinical significance, specifying how these findings could be practically applied in clinical settings and delineating steps for using NiTi devices and antibiotics in root canal treatment are important for the broader implementation of treatment strategies to patients.
The findings of the present study demonstrated that a significant pain reduction was achieved through the synergistic approach of NiTi mechanical preparation, ultrasonic irrigation and multi-antibiotic occlusion during root canal treatment of deciduous teeth. This combined methodology not only effectively mitigated postoperative pain but also enhanced overall treatment efficiency. The positive outcomes observed with the application of NiTi files, ultrasonic irrigation and multi-antibiotic closure in the management of periapical inflammation in primary teeth may signify its potential for broader clinical adoption in the future.
The present study analyzed the efficacy of the NiTi file, ultrasonic irrigation and multi-antibiotic closure approach in the clinical treatment of primary teeth with periapical inflammation. This method potentially holds promise for wider implementation and may contribute to the future advancement of contemporary clinical practices. Furthermore, the use of multiple antibiotic pastes as a treatment option for root canal closure in deciduous teeth offers an efficient treatment for patients in clinical settings.
Supplementary Material
Comparison of the pain degree on day 1 after root canal surgery among different treatment groups.
Comparison of the pain degree on day 3 after root canal surgery among different treatment groups.
Comparison of the pain degree on day 7 after root canal surgery among different treatment groups.
Acknowledgements
Not applicable.
Funding
Funding: This work was financially supported by the Southwest Medical University Youth Program (grant no. 2021ZKQN025) and Project of Stomatological Institute of Southwest Medical University (grant no. 2021XJYJS01).
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
ZZ and GF conceived the study, designed the study and drafted the original manuscript. ZZ analyzed the data and conducted the experiments. GF critically revised the manuscript and provided constructive feedback. ZZ and GF confirm the authenticity of all the raw data. All authors have read and approved the final version of the manuscript.
Ethics approval and consent to participate
All procedures performed in the study involving human participants were approved by The Medical Ethics Committee of The Affiliated Hospital of Southwest Medical University (approval no. 20200916002; Sichuan, China). The legal guardians of all patients provided written informed consent for participation in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
|
Nair PN: Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med. 15:348–381. 2004.PubMed/NCBI View Article : Google Scholar | |
|
Andreasen FM: Transient apical breakdown and its relation to color and sensibility changes after luxation injuries to teeth. Endod Dent Traumatol. 2:9–19. 1986.PubMed/NCBI View Article : Google Scholar | |
|
Liu D, Peng X, Wang S, Han Q, Li B, Zhou X, Ren B, Xu HHK, Weir MD, Li M, et al: A novel antibacterial resin-based root canal sealer modified by Dimethylaminododecyl Methacrylate. Sci Rep. 9(10632)2019.PubMed/NCBI View Article : Google Scholar | |
|
Chum JD, Lim DJZ, Sheriff SO, Pulikkotil SJ, Suresh A and Davamani F: In vitro evaluation of octenidine as an antimicrobial agent against Staphylococcus epidermidis in disinfecting the root canal system. Restor Dent Endod. 44(e8)2019.PubMed/NCBI View Article : Google Scholar | |
|
Zehnder M: Root canal irrigants. J Endod. 32:389–398. 2006.PubMed/NCBI View Article : Google Scholar | |
|
Chen Y, Li H, Li M, Yang L, Sun Q and Chen K: Analysis of survival and factors associated with failure of primary tooth pulpectomies performed under general anaesthesia in children from South China. Int J Paediatr Dent. 30:225–233. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Nagarathna C, Vishwanathan S, Krishnamurthy NH and Bhat PK: Primary molar pulpectomy using two different obturation techniques: A clinical study. Contemp Clin Dent. 9:231–236. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Jiang J, Sun J, Huang Z, Bi Z, Yu G, Yang J and Wang Y: The state of the art and future trends of root canal files from the perspective of patent analysis: A study design. Biomed Eng Online. 21(90)2022.PubMed/NCBI View Article : Google Scholar | |
|
Al-Obaida MI, Alzuwayer AA, Alanazi SS and Balhaddad AA: In Vitro analysis of the fatigue resistance of four single file canal preparation instruments. Materials (Basel). 15(688)2022.PubMed/NCBI View Article : Google Scholar | |
|
Topçuoğlu G, Topçuoğlu HS, Delikan E, Aydınbelge M and Dogan S: Postoperative pain after root canal preparation with hand and rotary files in primary molar teeth. Pediatr Dent. 39:192–196. 2017.PubMed/NCBI | |
|
Singh A, Purohit BM and Mittal P: Periodontal predicaments and associated risk factors among patients with schizophrenia. Neurology, Psychiatry and Brain Research. 32:36–41. 2019. | |
|
Divya DV, Ghanashyam PM, Naga RA, Venkata SR, Pavani RS and Santosh Kumar KVK: Triple antibiotic paste versus propolis: A clinical quest for the reliable treatment of periapical lesions in primary molars. Saudi Dental Journal. 9:34–39. 2019. | |
|
Wu D, Gao J, Hu X, Xiao Z, Huang Z, Zhang L, Chen X and He Y: Evaluation algorithm of root canal shape based on steklov spectrum analysis. Comput Math Methods Med. 2019(4830914)2019.PubMed/NCBI View Article : Google Scholar | |
|
Wang C, Xu P, Li X, Zheng Y and Song Z: Research progress of stimulus-responsive antibacterial materials for bone infection. Front Bioeng Biotechnol. 10(1069932)2022.PubMed/NCBI View Article : Google Scholar | |
|
Nakamura VC, Pinheiro ET, Prado LC, Silveira AC, Carvalho APL, Mayer MPA and Gavini G: Effect of ultrasonic activation on the reduction of bacteria and endotoxins in root canals: A randomized clinical trial. Int Endod J 51 Suppl. 1:e12–e22. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Klyn SL, Kirkpatrick TC and Rutledge RE: In Vitro comparisons of debris removal of the EndoActivatorTM System, the F File, Ultrasonic Irrigation, and NaOCl irrigation alone after hand-rotary instrumentation in human mandibular molars. J Endod. 36:1367–1371. 2010.PubMed/NCBI View Article : Google Scholar | |
|
Narayanan LL and Vaishnavi C: Endodontic microbiology. J Conserv Dent. 13:233–239. 2010.PubMed/NCBI View Article : Google Scholar | |
|
Cogulu D, Uzel A, Oncag O and Eronat C: PCR-based identification of selected pathogens associated with endodontic infections in deciduous and permanent teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 106:443–449. 2008.PubMed/NCBI View Article : Google Scholar | |
|
Pak JG and White SN: Pain prevalence and severity before, during, and after root canal treatment: A systematic review. J Endod. 37:429–438. 2011.PubMed/NCBI View Article : Google Scholar | |
|
Fischer NG, Münchow EA, Tamerler C, Bottino MC and Aparicio C: Harnessing biomolecules for bioinspired dental biomaterials. J Mater Chem B. 8:8713–8747. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Manzoori JL, Amjadi M, Soltani N and Jouyban A: Spectrofluorimetric determination of cefixime using terbium-danofloxacin probe. Iran J Basic Med Sci. 17:256–262. 2014.PubMed/NCBI | |
|
Schlenter WW, Blessing R, Pelz K and Benner U: Cefixime treatment in different bacterial infections in the ENT region. Infection. 18 (Suppl 3):S125–S128. 1990.PubMed/NCBI View Article : Google Scholar : (In German). | |
|
Mehrvarzfar P, Esnashari E, Salmanzadeh R and Fazlyab M and Fazlyab M: Effect of dexamethasone intraligamentary injection on post-endodontic pain in patients with symptomatic irreversible pulpitis: A randomized controlled clinical trial. Iran Endod J. 11:261–266. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Li X, Chen X, Wu J, Liu Z, Wang J, Song C, Zhao S, Lei H and Sun Y: Portable, rapid, and sensitive time-resolved fluorescence immunochromatography for on-site detection of dexamethasone in milk and pork. Foods. 10(1339)2021.PubMed/NCBI View Article : Google Scholar | |
|
Yu W, Tong J, Sun X, Chen F, Zhang J, Pei Y, Zhang T, Zhang J and Zhu B: Analysis of medication adherence and its influencing factors in patients with Schizophrenia in the Chinese Institutional Environment. Int J Environ Res Public Health. 18(4746)2021.PubMed/NCBI View Article : Google Scholar | |
|
Ahmed HM, Khamis MF and Gutmann JL: Seven root canals in a deciduous maxillary molar detected by the dental operating microscope and micro-computed tomography. Scanning. 38:554–557. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Siqueira JF Jr and Rôças IN: Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 34:1291–1301.e3. 2008.PubMed/NCBI View Article : Google Scholar | |
|
Williamson AE, Sandor AJ and Justman BC: A comparison of three nickel titanium rotary systems, EndoSequence, ProTaper universal, and profile GT, for canal-cleaning ability. J Endod. 35:107–109. 2009.PubMed/NCBI View Article : Google Scholar | |
|
Gulabivala K, Patel B, Evans G and Ng Y-L: Effects of mechanical and chemical procedures on root canal surfaces. Endodontic Topics. 10:103–122. 2005. | |
|
Alghazaly A and Al Habib L: Management of endodontic flare-up in the presence of periapical radiolucency: Case report and overview. Cureus. 15(e49719)2023.PubMed/NCBI View Article : Google Scholar | |
|
de Deus Moura Lde F, de Lima Mde M, Lima CC, Machado JI, de Moura MS and de Carvalho PV: Endodontic treatment of primary molars with antibiotic paste: A report of 38 cases. J Clin Pediatr Dent. 40:175–177. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Shariati A, Arshadi M, Khosrojerdi MA, Abedinzadeh M, Ganjalishahi M, Maleki A, Heidary M and Khoshnood S: The resistance mechanisms of bacteria against ciprofloxacin and new approaches for enhancing the efficacy of this antibiotic. Front Public Health. 10(1025633)2022.PubMed/NCBI View Article : Google Scholar | |
|
Scholar E: Minocycline. In: xPharm: The Comprehensive Pharmacology Reference. Enna SJ and Bylund DB (eds). Elsevier, New York, NY, pp1-6, 2007. | |
|
Ito IY, Junior FM, Paula-Silva FW, Da Silva LA, Leonardo MR and Nelson-Filho P: Microbial culture and checkerboard DNA-DNA hybridization assessment of bacteria in root canals of primary teeth pre- and post-endodontic therapy with a calcium hydroxide/chlorhexidine paste. Int J Paediatr Dent. 21:353–360. 2011.PubMed/NCBI View Article : Google Scholar |









