



Ependymoma with metastases to the gallbladder: A case report and literature review
- Authors:
- Published online on: December 21, 2023 https://doi.org/10.3892/ol.2023.14205
- Article Number: 72
-
Copyright: © Han et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
Introduction
Ependymoma is a neuroepithelial tumor that can originate from ependymal cells in the brain, the central canal of the spinal cord or the cortex. The incidence rate of ependymoma is low, accounting for 1.6–1.8% of all primary central nervous system tumors; it is more common in children, accounting for 5.2%, while it is ~4% in adults. The incidence rate in males is slightly higher than that in females (1.3:1) (1). The location of the tumor largely depends on the patient's age, with ~90% of pediatric ependymomas occurring in the intracranial region and 65% of adult tumors occurring in the spinal cord (2). Carcinomas commonly metastasize to the lymph nodes, lungs, bones, liver and brain. However, metastases to the gallbladder are rare and have only been reported minimally in the literature (3–5). In addition, primary tumors, such as hepatocellular carcinoma (6) and pancreatic cancer (7), may invade the gallbladder. However, ependymoma that metastasizes to the gallbladder has not been reported previously. In the present study, the case of a patient with metastatic ependymoma to the gallbladder who underwent cholecystectomy under general anesthesia with nerve block anesthesia was described. Furthermore, a review of the literature on this condition was provided in the present report.
Case report
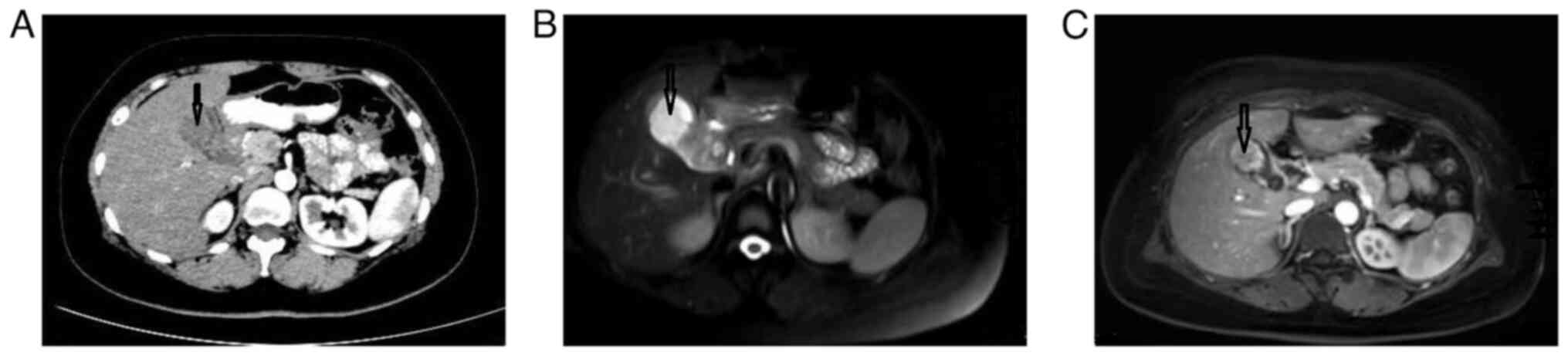
A 42-year-old female patient presented at Cangzhou People's Hospital (Cangzhou, China) in May 2022 due to the discovery of a gallbladder mass in an ultrasound examination 11 days prior. The patient underwent an enhanced spiral CT scan of the lower abdomen, which revealed irregular thickening of the gallbladder wall protruding into the cavity (May 2022). The enhancement progressively increased after administration of contrast agent, and there was an unclear boundary between the lesion and the liver (Fig. 1A). Based on these findings, the possibility of gallbladder cancer was considered. An abdominal MRI (May 2022) showed that the upper part of the gallbladder body was occupied, with significant enhancement on the enhanced scan. In addition, the cystic duct was dilated, indicating the presence of possible gallbladder malignant tumor lesions (Fig. 1B and C).
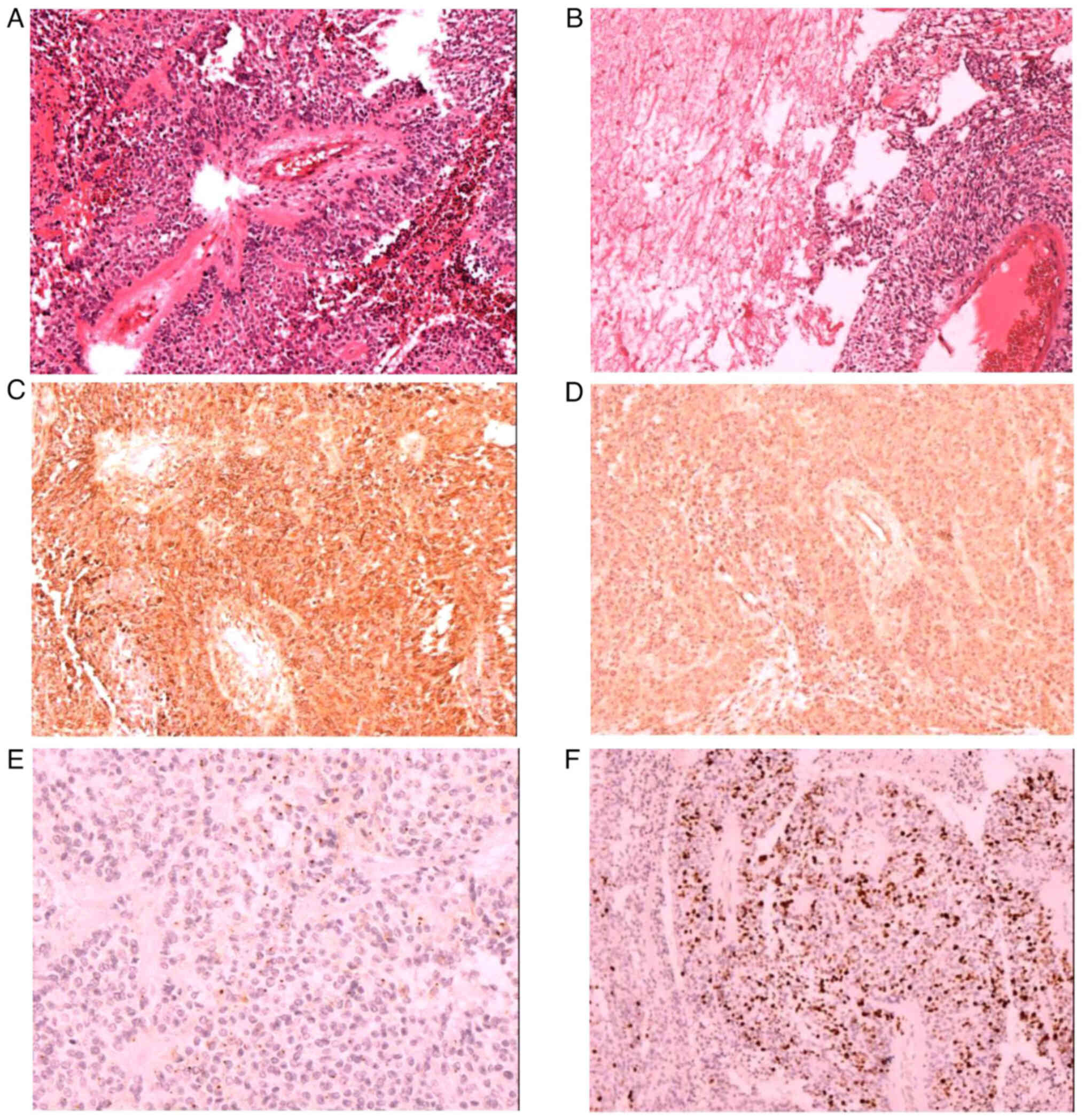
The patient had previously undergone a craniotomy at The Third Medical Center of the Chinese People's Liberation Army General Hospital (Beijing, China) for a right frontal lobe mass in 2017. The postoperative pathological report confirmed it as an anaplastic ependymoma [World Health Organization (WHO) grade III] (8) in the right frontal lobe. Under a microscope, tumor cells can be observed to be circular or elliptical in shape, with a false rosette like structure around the blood vessels (Fig. 2A). In addition, necrosis can be observed in the tumor tissue (Fig. 2B). Immunohistochemistry [performed using the Ventura BenchMark ULTRA (Roche Diagnostics) staining procedure; all reagents were from Roche Diagnostics] indicated that the mass was glial fibrillary acidic protein GFAP+ (cat. no. GM-0031; 1:100 dilution; Fig. 2C), partially S-100+ (cat. no. SM-0011; 1:100 dilution), Vimentin+ (cat. no. VM-0031; 1:100 dilution; Fig. 2D), EMA+ (cat. no. EM0-0041; 1:100 dilution; Fig. 2E), Olig2− (cat. no. ORM-0015; 1:100 dilution), Ki67 (10–20%; cat. no. KM-0021; 1:100 dilution; Fig. 2F), neuron-specific enolase+ (cat. no. NM-0019; 1:100 dilution) and D2-40− (cat. no. DM-0011; 1:100 dilution). Postoperative radiotherapy was administered.
In June 2022, the patient underwent cholecystectomy under general anesthesia with nerve block at Cangzhou People's Hospital (Cangzhou, China). Intraoperative exploration revealed adhesions between the omentum and gallbladder, with no thickening of the common bile duct and no palpable calculi. A medium-sized mass measuring ~5×3×3 cm was palpable at the bottom of the gallbladder, but it did not invade the surrounding tissues. Visual inspection indicated that the gallbladder had a size of 7×4×3 cm and had been previously incised. A mass, measuring 5×4×3 cm, was observed in the cyst at the bottom of the gallbladder, with a soft and tough cut surface and focal necrosis.
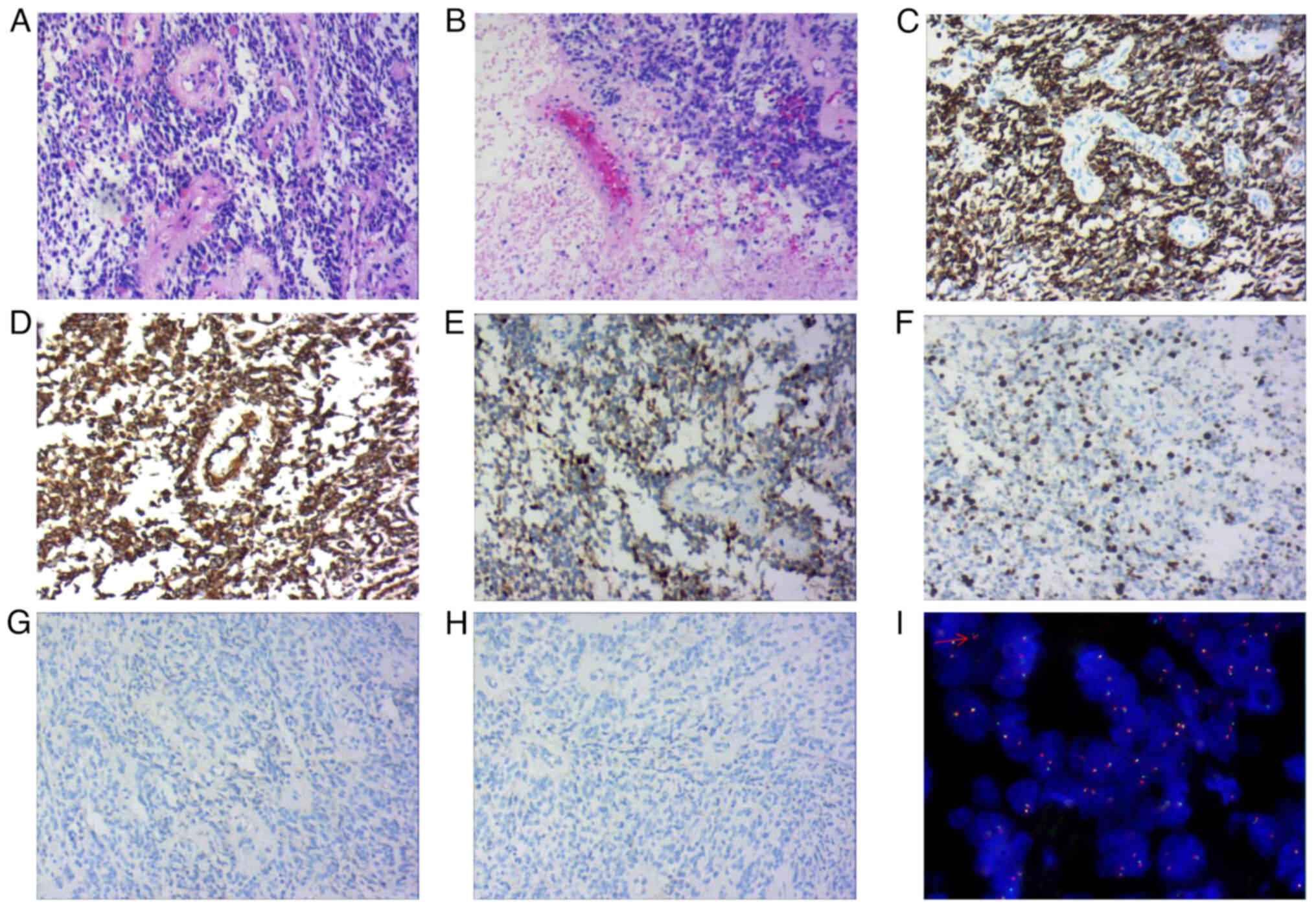
Histological examination (samples were prepared using the Ventura BenchMark ULTRA staining procedure; all reagents were from Roche Diagnostics) revealed the presence of round or oval monomorphic cells of uniform size within the tumor tissue. Numerous tumor cells formed a pseudo rosette-like structure around blood vessels. Immunohistochemistry (May 2022) results showed that the mass was GFAP+ (cat. no. GM-0031; 1:100 dilution), Vimentin+ (cat. no. VM-0031; 1:100 dilution), Ki67 (index ~10%; cat. no. KM-0021; 1:100 dilution), partially S-100+ (cat. no. SM-0011; 1:100 dilution), EMA− (cat. no. EM0-0041; 1:100 dilution), CD56+ (cat. no. CRM-0351; 1:100 dilution), neuron-specific enolase+ (cat. no. NM-0019; 1:100 dilution; all from Shanghai Jiehao Biotechnology Co., Ltd.), β-catenin+ (Qiagen; cat. no. BM-0267; 1:100 dilution) and cytokeratin− (CK; cat. no. CM-0641; 1:100 dilution; Shanghai Jiehao Biotechnology Co., Ltd.) (Fig. 3A-H). Molecular detection using the C11orf95 zinc finger translocation associated (ZFTA)-RELA proto-oncogene fusion probe indicated positive fluorescence in situ hybridization expression (Fig. 3I; Appendix S1). At the same time, tumor markers related to differential diagnosis (lymphatic tissue tumors, vascular-derived tumors, biliary epithelial tumors, myoepithelial derived tumors and neuroendocrine tumors), including leukocyte common antigen− (cat. no. LM-0032; 1:100 dilution), CD31− (cat. no. CM-0251; 1:100 dilution), CD34− (cat. no. CM-0271; 1:100 dilution), CK19− (cat. no. CM-0621; 1:100 dilution), SMA− (cat. no. AM-0051; 1:100 dilution), calponin− (cat. no. CM-0081; 1:100 dilution) and CD99− (cat. no. CM-0211; 1:100 dilution; all from Shanghai Jiehao Biotechnology Co., Ltd.) (May 2022), were investigated. Through these immunohistochemistry methods, diseases such as primary gallbladder adenocarcinoma, angiosarcoma and lymphoma were excluded.
The pathological diagnosis indicated metastatic anaplastic ependymoma of the gallbladder (WHO grade III). The patient was followed up for 10 months after surgery and received targeted treatment at another hospital (Tianjin Medical University Cancer Institute Hospital; Tianjin, China). At present, the tumor has metastasized to the lungs and bones.
Discussion
Ependymoma is a rare primary tumor of the central nervous system that arises from ependymal cells and primarily affects young adults and children (1). The most common site of occurrence is the fourth ventricle, followed by the central canal of the spinal cord (8). It rarely occurs outside the cranial or spinal cord, with the sacrococcygeal region being the most frequent extracranial location (9). Other sites of occurrence include the ovaries, mediastinum, uterine ligaments, uterine rectal space and omentum (9).
According to the 2016 WHO classification criteria, subependymomas and mucopapillary ependymomas are classified as grade I, ependymomas as grade II and anaplastic ependymomas as grade III (8). The key diagnostic features in terms of pathomorphology are perivascular pseudo rosette-like structures, nodular growth patterns and ependymal rosette-like structures or fissures. Mitotic figures are uncommon, while atypia is occasionally observed. Sex nuclei degeneration is frequently present and necrosis is relatively common (8).
In clinical practice, metastasis to the gallbladder is infrequent. Specifically, malignant melanoma is the most common primary tumor that metastasizes to the gallbladder, accounting for 15% of cases (10,11). Renal cell cancers, lung cancers, cervical cancers and breast cancers can also lead to secondary metastasis to the gallbladder, although they are less common (12). Only a small number of cases of metastasis to the gallbladder have been documented in the literature (12,13). Metastasis to the gallbladder typically presents with symptoms resembling acute/chronic cholecystitis or complaints such as abdominal pain (14–16).
There have been no reports of ependymoma metastasis to the gallbladder. Unlike previously reported cases (12), the present case was identified through physical examination. Due to the rarity of metastatic ependymoma in the gallbladder and the absence of specific clinical and imaging findings, diagnosis without a clear medical history has been challenging (12). Therefore, molecular biology and immunohistochemical evaluation are often necessary. Risk factors for dissemination and metastasis of ependymoma include younger age, incomplete tumor resection, high-grade or mucopapillary ependymoma and a higher tumor proliferation index, among others (17).
Patients with gallbladder metastasis may experience abdominal pain, cholangitis, bile peritonitis or cholestasis. Histopathological examination facilitates the establishment of a diagnosis, as abdominal imaging has limited diagnostic value. Due to the poor condition of the patient after gallbladder metastasis, palliative treatment was adopted with a focus on alleviating the patient's symptoms. One report indicated that gallbladder metastasis accounted for 4.8% of all gallbladder malignancies (18). The prognosis for patients with gallbladder metastasis who undergo radical resection is favorable. However, patients primarily presenting with acute cholecystitis as a result of gallbladder metastasis have a poorer prognosis (19). Clinicians should remain aware of gallbladder metastasis in patients with malignant tumors exhibiting biliary symptoms. The present study had certain limitations, mainly as the technology used could not provide detailed molecular typing of ependymoma, such as Yes-associated protein 1 fusion-positive and ZFTA fusion, which are closely associated with biological behavior and clinical prognosis (20).
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Authors' contributions
XYH and ZGZ were involved in the conception and design of the study; QMS and SS performed imaging analyses; HZL and SLH completed the FISH detection; XYH and ZGZ confirm the authenticity of all the raw data. All authors have read and approved the final version of the manuscript.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for the publication of any data and/or accompanying images.
Competing interests
The authors declare that they have no competing interests.
References
|
McGuire CS, Sainani KL and Fisher PG: Incidence patterns for ependymoma: A surveillance, epidemiology, and end results study. J Neurosurg. 110:725–729. 2009. View Article : Google Scholar : PubMed/NCBI | |
|
Wani K, Armstrong TS, Vera-Bolanos E, Raghunathan A, Ellison D, Gilbertson R, Vaillant B, Goldman S, Packer RJ, Fouladi M, et al: A prognostic gene expression signature in infratentorial ependymoma. Acta Neuropathol. 123:727–738. 2012. View Article : Google Scholar : PubMed/NCBI | |
|
Missori G, Serra F, Prestigiacomo G, Ricciardolo AA, Brugioni L and Gelmini R: Case report: Metastatic breast cancer to the gallbladder. F1000Res. 9:3432020. View Article : Google Scholar : PubMed/NCBI | |
|
Chung PH, Srinivasan R, Linehan WM, Pinto PA and Bratslavsky G: Renal cell carcinoma with metastases to the gallbladder: Four cases from the national cancer institute (NCI) and review of the literature. Urol Oncol. 30:476–481. 2012. View Article : Google Scholar : PubMed/NCBI | |
|
Zagouri F, Sergentanis TN, Koulocheri D, Nonni A, Bousiotou A, Domeyer P, Michalopoulos NV, Dardamanis D, Konstadoulakis MM and Zografos GC: Bilateral synchronous breast carcinomas followed by a metastasis to the gallbladder: Acase report. World J Surg Oncol. 5:1012007. View Article : Google Scholar : PubMed/NCBI | |
|
Ma Y, Li GY and Chen G: A case of long-term gallbladder metastasis after primary liver cancer surgery. Chinese J Surg. 59:22021. | |
|
Yu S, Wang TK, Chen BY, et al: Diagnosis and treatment of 2 cases of metastatic tumors of the gallbladder and literature review. J Hepatopancreatobiliary Surg. 30:32018. | |
|
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P and Ellison DW: The 2016 world health organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 131:803–820. 2016. View Article : Google Scholar : PubMed/NCBI | |
|
Chen YR, Lin JM, Li J, et al: Uterine broad ligament ependymoma: A case report and literature review. Progress Obstet Gynecol. 26:22017. | |
|
Lee YT: Breast carcinoma: Pattern of metastasis at autopsy. J Surg Oncol. 23:175–180. 1983. View Article : Google Scholar : PubMed/NCBI | |
|
Langley RG, Bailey EM and Sober AJ: Acute cholecystitis from metastatic melanoma to the gall-bladder in a patient with a low-risk melanoma. Br J Dermatol. 136:279–282. 1997. View Article : Google Scholar : PubMed/NCBI | |
|
Shah RJ, Koehler A and Long JD: Bile peritonitis secondary to breast cancer metastatic to the gallbladder. Am J Gastroenterol. 95:1379–1381. 2000. View Article : Google Scholar : PubMed/NCBI | |
|
Abdelilah B, Mohamed O, Yamoul R, Elkhiyat I, Al Bouzidi A, Alkandry S and Abdelkader E: Acute cholecystitis as a rare presentation of metastatic breast carcinoma of the gallbladder: A case report and review of the literature. Pan Afr Med J. 17:2162014. View Article : Google Scholar : PubMed/NCBI | |
|
Calafat P, de Diller AB and Sanchez C: Metástasis de carcinoma de mama en ileon-colon y vesicula biliar simulando enfermedades inflamatorias (Breast carcinoma metastasis in ileum-colon and gallbladder simulating inflammatory diseases). Rev Fac Cien Med Univ Nac Cordoba. 56:123–127. 1999.(In Spanish). PubMed/NCBI | |
|
Borst MJ and Ingold JA: Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast. Surg. 114:637–641. 1993.PubMed/NCBI | |
|
Murguia E, Quiroga D, Canteros G, Sanmartino C, Barreiro M and Herrera J: Gallbladder metastases from ductal papillary carcinoma of the breast. J Hepatobiliary Pancreat Surg. 13:591–593. 2006. View Article : Google Scholar : PubMed/NCBI | |
|
Markelov A, Taheri H, Vunnamadala K and Ibrahim G: Biliary dyskinesia as a rare presentation of metastatic breast carcinoma of the gallbladder: A case report. Case Rep Pathol. 2011:8065702011.PubMed/NCBI | |
|
Yoon WJ, Yoon YB, Kim YJ, Ryu JK and Kim YT: Metastasis to the gallbladder: A single-center experience of 20 cases in South Korea. World J Gastroenterol. 15:4806–4809. 2009. View Article : Google Scholar : PubMed/NCBI | |
|
Doval DC, Bhatia K, Pavithran K, Sharma JB, Vaid AK and Hazarika D: Breast carcinoma with metastasis to the gallbladder: An unusual case report with a short review of literature. Hepatobiliary Pancreat Dis Int. 5:305–307. 2006.PubMed/NCBI | |
|
Bale TA and Rosenblum MK: The 2021 WHO classification of tumors of the central nervous system: An update on pediatric low-grade gliomas and glioneuronal tumors. Brain Pathol. 32:e130602022. View Article : Google Scholar : PubMed/NCBI |









