



Gastric granular cell tumor: A case report and literature review
- Authors:
- Published online on: June 27, 2024 https://doi.org/10.3892/ol.2024.14536
- Article Number: 403
-
Copyright: © Li et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
Introduction
Gastric granular cell tumors (GCTs) are exceedingly rare. GCTs in general represent an uncommon subset of soft-tissue neoplasms. The origin of the tissue remains controversial, although an accumulating number of studies have suggested that it may have originated via Schwann cell differentiation (1–3). In a previous retrospective analysis of 410,000 surgical specimens collected over a 32-year period from the National Naval Medical and Dental Centers (Bethesda, USA) and the Georgetown University Hospital (Washington, USA) Lack et al (4) reported that the overall incidence of GCTs was 0.03%. GCTs can occur in various parts of the body, although they most commonly arise in the skin and subcutaneous tissues of the head, neck, trunk, limbs and vulva. Gastrointestinal involvement accounts for only 4–6% of all GCTs (5). However, this involvement primarily affects the esophagus and colorectum, with gastric occurrences being particularly scarce. Mobarki et al (6) previously reported 42 GCTs cases, including resections and biopsies identified in electronic medical records of the Pathology Department in the University Hospital of Saint Etienne (Saint Etienne, France) over a 21-year period. Only 8 cases (7 esophageal and 1 right colonic) in the gastrointestinal tract were found. In another study, An et al (7) reported 98 cases of GCTs in the gastrointestinal tract, comprising 73 esophageal (75%), 21 colorectal (21%) and 4 gastric (4%) cases.
The detection of gastric GCTs has been facilitated by the use of endoscopy and endoscopic ultrasonography (EUS). In endoscopy, GCTs are typically sessile, small in size, yellowish-white and covered by a normal mucous membrane (8). The histology of GCTs is characterized by abundant eosinophilic granules in the cytoplasm and immunohistochemistry staining yielding positivity for S-100, CD68 and transcription factor SOX-10 (SOX-10) (9). Similar to the majority of subepithelial lesions (SELs), GCTs are difficult to obtain sufficient quantities of tumor tissues from using traditional gastroscopy biopsy techniques, as the tumor surface is covered with normal mucosa, making disease diagnosis difficult (10). EUS can be used to adequately observe the characteristics of SELs, including location, size, echo and boundary, facilitating the diagnosis and treatment of such submucosal lesions (11). The majority of gastric GCTs are benign and have favorable prognosis, but occasionally they may exhibit aggressive characteristics, such as local recurrence or distant metastasis (12,13). The treatment method of gastric GCTs remains unclear, with possibilities including endoscopic resection and traditional surgical resection. Due to its malignant potential, a review of such gastric GCT cases is necessary (14).
The present study documents the case of a 52-year-old man with a gastric body GCT that was completely excised by endoscopic submucosal dissection (ESD) and showed immunohistochemical positivity for S100, with CD34 expression surrounding the gastric GCT cells. The patient recovered well postoperatively. The aim of the present case was to contribute to the diagnostic and therapeutic understanding of gastric GCTs.
Case report
In May 2023, a 52-year-old man visited the Gastroenterology Clinic of the People's Hospital of Putuo District (Zhoushan, China) due to upper abdominal fullness over the last week. No significant abdominal pain, nausea, vomiting, diarrhea, constipation, hematemesis, melena, or cessation of flatus or stool passage was reported. Gastroscopy indicated a mucosal elevation in the anterior wall of the lower part of the gastric body (Fig. 1A). A 20-MHz EUS probe (model no. IM-02M-01; InnerMedical, Co., Ltd.; Table I) revealed a hypoechoic mass in the third layer (submucosal layer), measuring 10.34×7.06 mm, with uniform internal echoes and distinct boundaries. The remaining layers displayed clear and intact echogenicity (Fig. 1B). Under gastroscopy, the surface mucosa appeared normal, without features of low-grade dysplasia, high-grade dysplasia or early carcinoma, such as red discoloration of the mucosal surface, depressed lesions or mucosal ulcers. The lesion was preliminarily diagnosed as a submucosal tumor, such as a leiomyoma, gastrointestinal stromal tumor (GIST), lipoma, schwannoma or neuroendocrine tumor. Abdominal computed tomography (Aquilion 16; Canon Medical Systems Corporation; Table I) showed a localized nodular elevation on the greater curvature of the stomach body that was ~8 mm in diameter, with mild continuous enhancement post-contrast (Fig. 1C). No enlarged lymph nodes were observed around the stomach. Laboratory investigations revealed that this patient presented with positive fecal occult blood. Other tests, including complete blood count, coagulation profile, renal function and tumor markers (such as chromogranin A, carcinoembryonic antigen and carbohydrate antigen 19–9), were all found to be within the normal limits. There was also no history of esophageal cancer, gastric cancer, intestinal cancer or gastrointestinal granulosa cell tumors in family members.
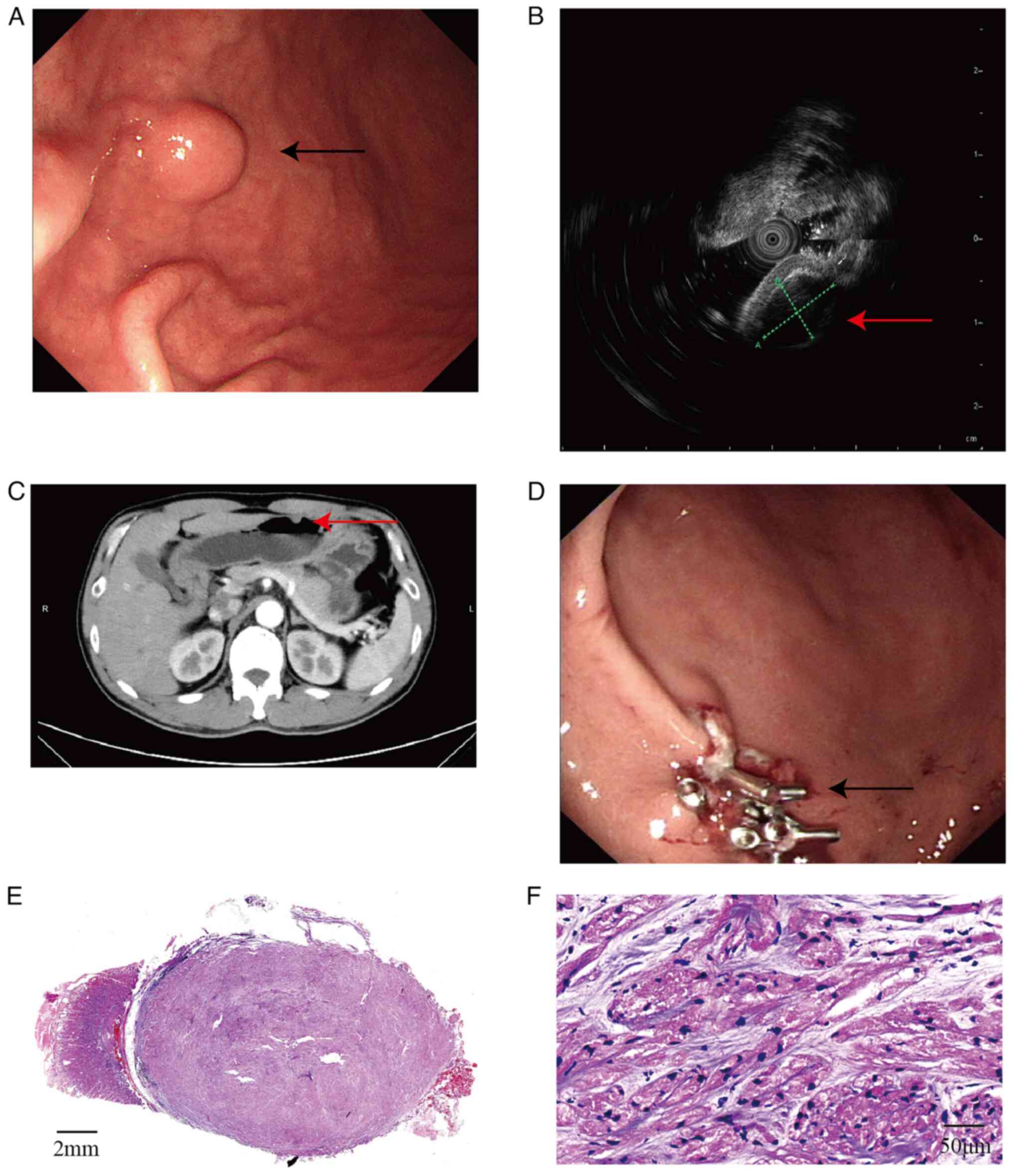
The patient was therefore admitted to the People's Hospital of Putuo District in June 2023 for further diagnosis and treatment, with a provisional diagnosis of a gastric space-occupying lesion. Subsequently, 2 days later, ESD was performed. After verifying patient information and successful intubation under general anesthesia, a polypoid elevation was observed in the stomach body. The surface mucosa was slightly congested. After circumferential marking, indigo carmine and saline were injected submucosally for elevation. The lesion was well lifted and the surrounding mucosa was incised using a Dual knife (KD-650L; Olympus Corp.). Submucosal dissection was progressively performed using Dual and insulation-tipped diathermic knife (KD-611L; Olympus Corp.). The lesion was completely excised using a snare. The operative site showed no perforation. Visible vessels on the wound surface were coagulated with hemostatic forceps, before the local surface was closed using titanium clips (Fig. 1D). Post-operation, to prevent complications and promote wound healing, the patient was administered 1.5 g cefuroxime sodium twice daily for 2 days as a preventive measure against infection. Additionally, a single dose of 80 mg carbazochrome sodium sulfonate was administered on the day of surgery to facilitate hemostasis, and 60 mg omeprazole was prescribed twice daily for two days to suppress gastric acid production. The patient recovered well and was discharged 3 days after surgery. The last time the patient visited the Gastroenterology Outpatient Clinic for a follow-up was 1 month later in July 2023, and there was no abdominal pain or distention. A follow-up visit was recommended 3–6 months after discharge; however, the patient has not yet scheduled this appointment. During the telephone follow-up conversation after 6 and 10 months of the operation, the patient reported that the symptoms had been relieved.
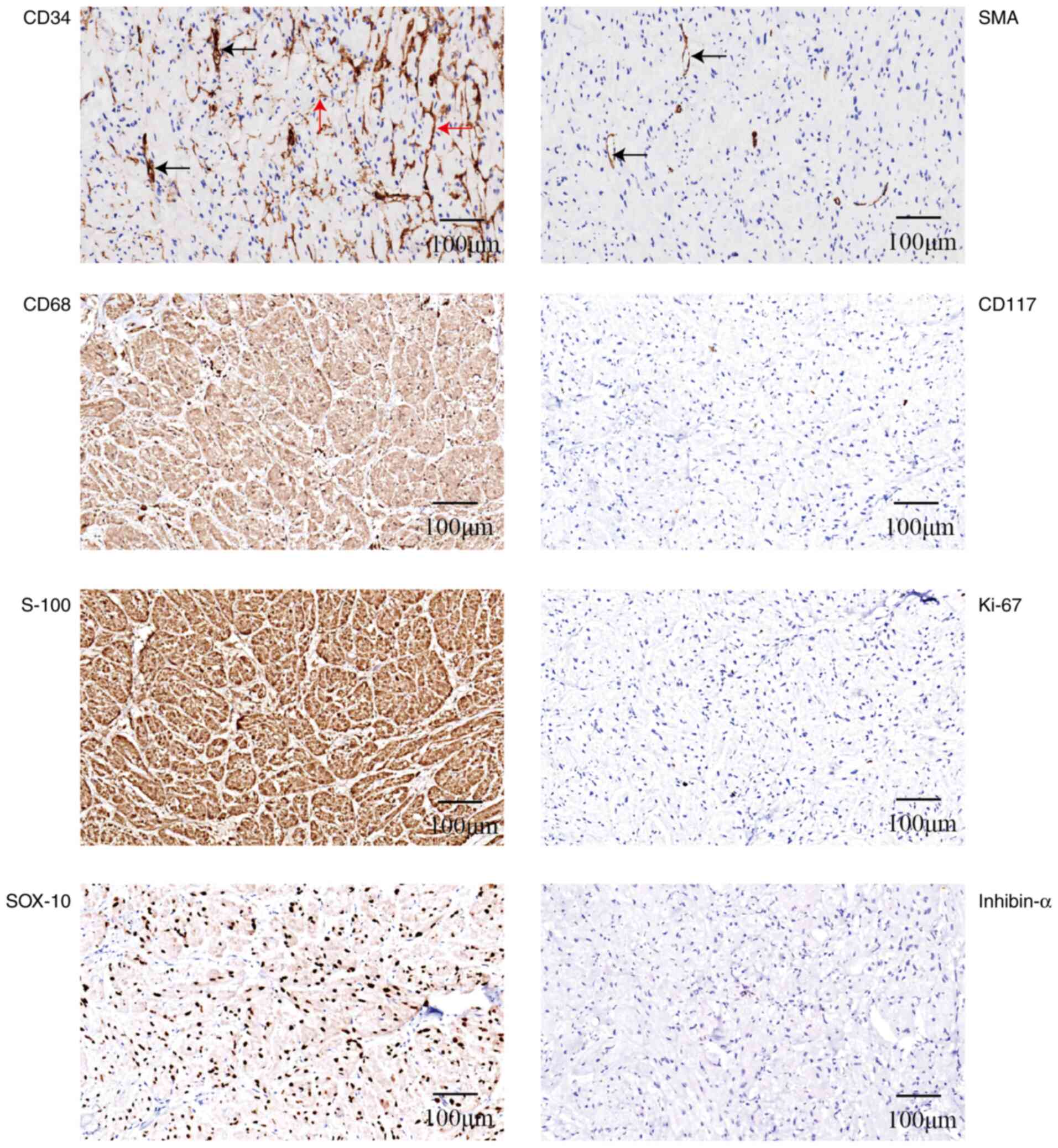
In terms of the pathology, the tumor was located in the submucosal layer and was nodular, with a gray-yellow cut surface and clear boundaries. Microscopically, tumor cells were arranged in bundles, nests and sheets, where the stroma was predominantly clear, with a loose matrix containing basophilic fibrous material and minimal blood vessel proliferation. The tumor cells were oval or polygonal with abundant eosinophilic granular cytoplasm. The nuclei were small, hyperchromatic, oval, short spindle-shaped and occasionally angular, with inconspicuous nucleoli (Fig. 1E and F). Immunohistochemistry revealed the following staining results: CD117(−), Ki-67 (low expression, <1%), smooth muscle actin (SMA)(−), S-100(+), SOX-10(+), CD68(+) and inhibin-α(−). CD34 staining was negative in the tumor cells but positive in the cells surrounding the tumor cell nests (Fig. 2). Tumor cells arranged in sheets and nests contained a large number of eosinophilic granules in the cytoplasm and expressed S-100 and CD68. These features closely resembled the GCTs commonly found in the skin, distinguishing them from neuroendocrine neoplasms. The negative expression of SMA and CD117 effectively ruled out the possibility of a gastric leiomyoma or GIST. Furthermore, the cells lacked characteristics such as a spindle shape, nuclear pleomorphism, prominent nucleoli, a high nuclear-to-cytoplasmic ratio, necrosis and significant mitoses. As the characteristics aligned with the internationally recommended Fanburg-Smith criteria (15) for diagnosing benign and malignant GCTs, the final diagnosis was of a benign gastric GCT. In the follow-ups until May 2024, the patient's symptoms have improved; however, due to work commitments, a visit to the hospital for a CT scan and gastroscopy review is temporarily not possible.
Hematoxylin and eosin staining (H&E), and immunohistochemistry
For H&E staining, the tissues were first fixed in a 10% formaldehyde solution for a period of 24 h at room temperature. After that, they were subjected to a dehydration process and subsequently embedded in paraffin. Next, they were cut into 4-µm thick sections. These sections underwent a dewaxing procedure utilizing xylene and ethanol before being thoroughly rinsed with water. The prepared sections were then sequentially stained with hematoxylin for 8 min and eosin dyes for 1 min at room temperature. Subsequently, the slices were observed under a light microscope.
S100 (cat. no. CSM-0101), CD34 (cat. no. CCM-0550), CD68 (cat. no. CCM-0701), SOX-10 (cat. no. CSR-0180), SMA (cat. no. CAM-0191), Ki-67 (cat. no. CKM-0032) and α-inhibin (cat. no. CIM-0151) antibodies were purchased from Celnotve Biotechnology, Co., Ltd. CD117 (cat. no. YR145) was purchased from MXB Biotechnology; Beijing Strong Biotechnologies. Paraffin sections of tissues were cut into 4-µm thick sections and mounted onto slides. After deparaffinization, rehydration and blocking endogenous peroxidase activity with 3% hydrogen peroxide for 10 min at room temperature, the slides were incubated with the appropriate aforementioned primary antibody (1:100) for 12 h at 4°C in a humidified chamber. Subsequently, the slides were incubated with the secondary antibody (cat. no. SD3003; Celnotve Biotechnology, Co., Ltd.) for 30 min at room temperature, and then incubated with the DAB chromogenic solution (cat. no. SD3004; Celnotve Biotechnology, Co., Ltd.) for 5 min. Finally, counterstaining was achieved through a 3-min incubation with hematoxylin at room temperature. After the staining was completed, a light microscope was used to observe the slides.
Literature review
For the literature review, the key words ‘gastric granulosa cell tumor’, ‘gastrointestinal granulosa cell tumor’, ‘digestive tract granulosa cell tumor’ and ‘granular cell tumor’ were searched for in PubMed data (https://pubmed.ncbi.nlm.nih.gov/) recorded between 1970 and 2024, and the English full-text study was obtained. Inclusion criteria were as follows: Case reports of gastric GCTs. Exclusion criteria were as follows: Articles for which full text could not be obtained. The literature was then reviewed, and the clinical and pathological characteristics of 42 gastric GCT cases were summarized, including country, sex, age, symptoms, location, size, immunohistochemistry results, treatment methods, follow-up information and outcome (Table II) (16–48).
Discussion
The histopathophysiology of GCTs remains unclear. Initially identified in 1926 by Abrikossoff (49) in five cases of tongue tumors, the tumor cells were found to be strikingly similar to skeletal muscle cells, rendering them being described as ‘granular cell myoblastomas’ at the time. In subsequent studies, the presence of S100 positivity, coupled with the complex granular and lysosomal ultrastructure observed under electron microscopy, suggested a potential differentiation towards Schwann cells (1,2). However, previous genetic studies on GCT cells did not demonstrate monosomy or deletions in the long arm of chromosome 22, a characteristic differing from that of schwannomas (15). Additionally, reports of S100-negative granular cell tumors have emerged (50–52). Therefore, the histopathophysiology of GCTs remains to be fully elucidated, necessitating further research. In the present gastric GCT case, CD34 expression was observed, but not in the tumor cells themselves; immunohistochemistry showed CD34-positive cells or matrix surrounding the tumor cells or nests, with SMA highlighting only a small vascular component within the tumor tissue. Previous studies have confirmed the specificity of glucose transporter protein 1 and epithelial membrane antigen for perineurial cells, whereas CD34 appeared to be immunoreactive to endoneurial fibroblasts (53). Díaz-Flores et al (54) previously observed CD34-positive interstitial cells around S100-positive Schwann cells. The present findings corroborate this observation, potentially suggesting a Schwann cell origin for GCTs. However, whether the CD34-positive cells are reactive or are part of the tumor, akin to the bidirectional differentiation that is commonly observed in breast fibroadenomas and salivary gland tumors, warrants further investigation.
From the present literature review, it was found that GCTs are mostly solitary, but can also present as multiple tumors in the same body (22,31,32,46,48) or involve multiple organs (25,29,31,32,35,42,46). Gastric GCTs typically involve the esophageal or colorectal regions. The site of gastric GCT occurrence shows no predilection and can occur in the cardia, body and antrum. The age of onset varies widely, with the mean age of patients with GCTs being 48 years (median, 50 years; range, 16–76 years). There is also no significant sex predisposition (18 males and 22 females). Among the 42 cases of gastric GCT recorded, there were 12 African and 12 Japanese individuals, which may suggest a higher prevalence of GCTs among these individuals. According to Patti et al (33), gastric GCTs are typically diagnosed in individuals aged between 40 and 60 years, with no specific sex predisposition. However, do seem to be ethnic considerations, since the majority of instances were observed in the Japanese population. Gastric GCTs lack a specifically defined set of clinical symptoms and laboratory findings. Patients with gastric GCTs will typically present with abdominal fullness, discomfort, abdominal pain or indigestion. Gastric GCTs are frequently discovered incidentally during imaging, gastroscopy or other surgeries. In the present case, the patient was a 52-year-old man who presented with abdominal fullness, and whose nodule was subsequently discovered during endoscopy. When ulcerated, the tumors may present with gastrointestinal bleeding. In addition, gastric GCTs can coexist with other diseases, such as gastric adenocarcinoma, esophageal cancer and gastric ulcers, manifesting symptoms of the concurrent diseases.
Endoscopically, gastric GCTs are typically covered with yellow, white or normal mucosa, presenting as polypoid or hemispherical protrusions into the stomach, and are mostly sessile. Macroscopically, they appear as well-demarcated, firm submucosal nodules, occasionally involving the muscularis propria or serosa. A number of patients do present with multiple nodules, with a total of 48 gastric GCTs studied in 42 patients. The location of 39 nodules was clearly defined, 27 of which were submucosal and 12 of which involved the serosa or muscle layer. The typical size is small, with 79% being <2 cm in size and the largest reaching 7 cm (13). The application of magnifying endoscopy or chromoendoscopy in SELs may be limited due to the normal mucosal covering (55). However, EUS is effective in characterizing the features of SELs (such as location, size, echo pattern and boundaries), aiding in narrowing the differential diagnoses and assessing the feasibility of endoscopic resection (11). Gastric GCTs on EUS typically present as uniform, hypoechoic lesions originating from the second or third layer (mucosal or submucosal) and occasionally from the fourth layer (if involving the muscularis propria). According to a retrospective study on SELs by Kida et al (56), besides GCTs, neuroendocrine tumors, lipomas and GISTs can also originate from the third layer. Apart from lipomas, which typically show hyperechoic features, GISTs, neuroendocrine tumors, leiomyomas and schwannomas can also present as hypoechoic. Abdominal computed tomography can be used to image well-demarcated intramural nodules with insignificant or mild enhancement, in addition to evaluating the overall condition of surrounding organs and lymph nodes. The EUS examination of the present case revealed a distinct, hypoechoic nodule positioned in the third layer, indicating the feasibility of resection via ESD.
However, distinguishing gastric GCTs from other submucosal tumors is challenging using imaging techniques alone. A definitive diagnosis typically requires pathological confirmation. Unlike epithelial tumors, due to the coverage of a normal mucosa, traditional endoscopic forceps biopsies, even with multiple attempts at the same site, will frequently fail to provide an accurate diagnosis of a gastric GCT. A EUS-guided fine-needle aspiration biopsy can yield satisfactory tumor tissue samples for diagnosis (10). In the present case, the gastric GCT was located in the submucosa, with normal mucosa on the surface, similar to most gastric GCTs.
Histologically, gastric GCTs are comprised of large polygonal or oval cells laden with abundant eosinophilic granules. The tumor margins can be well defined or infiltrative. Pareja et al (57) previously found that loss-of-function mutations in the ATPase H+ transporting accessory protein 1 (ATP6AP)1 and ATP6AP2 genes may be the driving factors of GCT through whole-exome sequencing and targeted sequencing of GCT. This finding suggested that intracellular vesicles found in GCT are acidic cytoplasmic granules that have accumulated due to vesicle acidification impairments. Immunohistochemically, apart from being consistently S100-positive (100%) and exhibiting mild Ki-67 positivity (<10%; 100%), they can also express CD68, SOX10, CD56, Nestin and inhibin (7,9). The tumors are typically negative for CD34, CD117, SMA and human melanoma black 45. Na et al (58) previously studied the immunohistochemical expression profile of 30 cases of colorectal GCT, before finding that the tumors were positive for S-100 (100%), CD68 (100%), neuron-specific enalase (100%), Nestin (100%), SOX-10 (100%), Ki-67 <1% (100%), CD56 (93%), synaptophysin (93%), calretinin (53%), CD163 (23%), CD57 (21%), p53 (32%) and inhibin-α (17%). In another previous study, An et al (7) found that the gastric GCTs were positive for S-100 (100%), CD56 (100%), SOX10 (100%), CD68 (67%) and inhibin-α (33%). However, in the present case, S-100, CD68 and SOX10 staining was positive, whereas inhibin-α staining was negative. Inhibin, a polypeptide hormone, is secreted by the granulosa cells of the ovary and the Sertoli cells of the testis (59). Inhibin negatively regulates the synthesis of follicle-stimulating hormone and the secretion of anterior pituitary, regulating gonad function (60), and its expression is closely associated with the differentiation of sex cells and steroid cells (61). While numerous studies have documented the presence of positive expression of inhibin-α in GCTs located in various parts of the body (62–64), other two studies revealed that only 52 or 17% of GCTs, respectively, exhibited positive inhibin-α expression (7,58). Currently, the precise role of inhibin-α expression in cell differentiation and the pathogenesis of GCTs remains enigmatic. Taban et al (9) also previously noted CD34 expression within the tumor, which appeared to be more pronounced at the periphery. Special periodic acid-Schiff staining can be used to reveal cytoplasmic granules (43). Gastric GCTs, due to their rich cytoplasm and granules, can be misdiagnosed as perivascular epithelioid cell tumors, which express both muscular and melanocytic markers (65). In addition, gastric GCTs typically present as non-neoplastic lesions, such as histiocytic aggregates. Diagnostic differentiation is also required from S100-expressing schwannomas, which exhibit distinct Antoni A and B areas, and are frequently accompanied by a lymphocyte cuff that is lacking abundant cytoplasmic granules (66). The most common submucosal tumors in the stomach, GISTs, are predominantly located in the muscularis layer and express CD117, GIST1 and CD34 (67). However, the pattern of CD34 expression surrounding tumor cell nests in GCTs distinguishes them from the expression CD34 characteristics observed in GISTs.
Although the majority of gastric GCTs (98%) are benign, there have been reports of malignant gastric GCTs (13). A previously reported 64-year-old female patient with a gastric tumor exhibiting S100-positive eosinophilic granular cells, atypical giant nuclei and mitotic figures was found to relapse 2 years later. Although an elevated Ki-67 index, necrosis and/or mitotic activity are frequently associated with malignant behavior, metastasis remains the only definitive sign of malignancy. Fanburg-Smith et al (15) previously studied 73 GCT cases and proposed the following six diagnostic criteria for differentiating benign GCTs from malignant GCTs: i) Necrosis; ii) spindle cell morphology; iii) nuclear pleomorphism; iv) prominent nucleoli; v) high nuclear-cytoplasmic ratio; and vi) increased mitotic activity (>2 mitoses per 10 high-power fields at ×200 magnification). Tumors meeting three or more of the aforementioned criteria are classified to be histologically malignant GCTs, whilst those meeting only one or two of the criteria would be considered atypical GCTs. However, there have been reports of histologically benign GCTs with metastases (2). Machado et al (68) suggested abandoning the distinction between benign and atypical GCTs, since they rarely metastasize and those that do, typically occur as a result of local recurrence due to incomplete resection. Instead, GCTs with various unfavorable histological features should be labeled as ‘GCTs with increased risk of metastasis’, rather than ‘malignant GCTs’. The tumor cells in the present case had pycnotic nuclei, inconspicuous nucleoli, a low nucleus-to-cytoplasm ratio, no nuclear division, no pleomorphism or fusiform cells, no necrosis and Ki-67 <1%. Abdominal computed tomography showed no abnormal lymph nodes around the stomach. The patient's symptoms have been significantly relieved, as assessed at 10 months post-surgery. These characteristics are in line with the diagnosis of a benign GCT.
A consensus on the treatment of gastric GCTs has not yet been fully established. In the present literature review, it was found that surgical excision was performed in 30 patients, including partial gastrectomy, wedge resection and local excision. In total, 3 patients underwent a total gastrectomy due to suspected lymph node metastasis, multiple gastric GCTs or concurrent adenocarcinoma. Endoscopic resections were performed in 9 patients, where, except for the malignant GCT that recurred after 2 years, there were no recurrences or metastases during the follow-up period. According to the 2022 European Society of Gastrointestinal Endoscopy (ESGE) guidelines (69), asymptomatic gastric GCTs with a clear diagnosis should not be monitored. If the diagnosis is unclear, endoscopic monitoring should be performed at 3–6 months, then every 2–3 years for lesions <10 mm in diameter and every 1–2 years for lesions 10–20 mm in diameter. For lesions >20 mm in diameter, ESGE recommends monitoring with endoscopy and EUS at 6 months, then every 6–12 months thereafter. However, challenges remain in diagnosing and monitoring compliance, since <2% of cases show potentially malignant biological behavior in gastric GCTs (70). Ryu et al (71) previously conducted a retrospective analysis of 35 cases of esophageal GCT that underwent endoscopic resection, which revealed that diagnostic endoscopic resection of submucosal tumors not only aids in a clear diagnosis, but can also serve certain therapeutic effects. Additionally, it was noted that various methods of endoscopic resections conferred no significant difference on therapeutic outcomes. Endoscopic mucosal resection (EMR) was originally introduced clinically for gastric lesions in 1984 by Tada et al (72) as a ‘strip biopsy’, which evolved into ESD, a variant of EMR (73). The majority of the 42 cases of gastric GCT in the present literature review were benign, where 77% were ≤2 cm in size. There was no recurrence in the 9 cases of endoscopic resection. Kahng et al (74) previously examined 25 patients with gastrointestinal GCT, totaling 27 gastrointestinal GCT tumors. Specifically, 20 were diagnosed in the esophagus, 5 in the stomach and 2 in the colon. All GCTs were resected endoscopically, with a median size of 10 mm. The mean follow-up period was 15 months, during which there were no recurrences. Endoscopic resection was therefore considered a safe and effective treatment for this condition. Another study by Yasuda et al (5) reviewed 12 cases of 34 gastric GCTs that underwent endoscopic resection. In total, 75.6% of tumors showed a diameter of ≤2 cm and no local recurrence was observed. It was therefore concluded that endoscopic resection is a viable treatment option. Of the 42 patients included in the present review, 9 underwent an endoscopic resection. Except for 1 patient whose tumor size was 2.5 cm, the other 8 patients all had tumors ≤2 cm in diameter. In addition, with the exception of 2 cases in which the location of the tumor was not disclosed, the tumors in the other 7 patients were located in the submucosa and did not invade the muscle layer. There was no recurrence after surgery. Therefore, it could be suggested that endoscopic resection is a feasible treatment option for gastric GCTs ≤2 cm, provided they do not involve the muscularis propria or have normal submucosal lifting during surgery. Otherwise, a combination of tumor removal and partial gastric wedge resection may be considered, including ≥1 cm of the normal tissue (33). Due to the rarity of the malignant gastric GCT cases, a complete tumor resection with clear margins is necessary, although evidence for lymph node dissection remains inconclusive.
In conclusion, GCTs are rare. The presence of CD34-positive interstitial cells surrounding S100-positive tumor cells in GCTs indicate that these cells are part of the tumor, providing evidence for the Schwann cell origin of gastric GCTs. The combination of EUS and endoscopic needle biopsy can enhance the diagnostic accuracy for gastric GCTs. The majority of gastric GCTs are benign and <2 cm in size, making endoscopic resection (such as EMR and ESD) a viable treatment option.
Acknowledgements
Not applicable.
Funding
The present case was supported by a grant from the Project of the Science and Technology Bureau of Putuo District of Zhoushan City (grant no. 2021GY304).
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
HXL diagnosed this case and managed the article design. MZ completed the immunohistochemistry. HXL and MZ collected data and obtained medical images. HZ analyzed the data and wrote the paper. YYZ analyzed the data. HXL and HZ reviewed, verified and confirm the authenticity of all the raw data. All authors have read and approved the manuscript.
Ethics approval and consent to participate
Ethics approval (approval no. 2024002KYLW) was obtained from the Ethics Committee of People's Hospital of Putuo District (Zhoushan, China) and an informed consent statement for participation was obtained from the patient.
Patient consent for publication
Written informed consent for publication was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
References
|
Stefansson K and Wollmann RL: S-100 protein in granular cell tumors (granular cell myoblastomas). Cancer. 49:1834–1838. 1982. View Article : Google Scholar : PubMed/NCBI | |
|
Ordonez NG and Mackay B: Granular cell tumor: A review of the pathology and histogenesis. Ultrastruct Pathol. 23:207–222. 1999. View Article : Google Scholar : PubMed/NCBI | |
|
Santos C, Araújo AV, Contente H and Branco C: Gastric granular cell tumour, a rare entity. BMJ Case Rep. 12:e2275102019. View Article : Google Scholar : PubMed/NCBI | |
|
Lack EE, Worsham RGF, Callihan MD, Crawford BE, Klappenbach S, Rowden G and Chun B: Granular cell tumor: A clinicopathologic study of 110 patients. J Surg Oncol. 13:301–316. 2006. View Article : Google Scholar | |
|
Yasuda A, Yasuda T, Imamoto H, Hiraki Y, Momose K, Kato H, Iwama M, Shiraishi O, Shinkai M, Imano M and Kimura Y: A case of a gastric granular cell tumor preoperatively diagnosed and successfully treated by single-incision laparoscopic surgery. Surg Case Rep. 6:442020. View Article : Google Scholar : PubMed/NCBI | |
|
Mobarki M, Dumollard JM, Col PD, Camy F, Peoc'h M and Karpathiou G: Granular cell tumor a study of 42 cases and systemic review of the literature. Pathol Res Pract. 216:1528652020. View Article : Google Scholar : PubMed/NCBI | |
|
An S, Jang J, Min K, Kim MS, Park H, Park YS, Kim J, Lee JH, Song HJ, Kim KJ, et al: Granular cell tumor of the gastrointestinal tract: Histologic and immunohistochemical analysis of 98 cases. Hum Pathol. 46:813–819. 2015. View Article : Google Scholar : PubMed/NCBI | |
|
Radaelli F and Minoli G: Granular cell tumors of the gastrointestinal tract: Questions and answers. Gastroenterol Hepatol (N Y). 5:798–800. 2009.PubMed/NCBI | |
|
Taban SM, Barna RA, Dema AL, Ratiu IM, Popa O and Plopeanu AD: Unexpected diagnosis for a gastric polyp: Granular cell tumor: Case report and review of the literature. Exp Ther Med. 21:5362021. View Article : Google Scholar : PubMed/NCBI | |
|
Sekine M, Asano T and Mashima H: The diagnosis of small gastrointestinal subepithelial lesions by endoscopic ultrasound-guided fine needle aspiration and biopsy. Diagnostics (Basel). 12:8102022. View Article : Google Scholar : PubMed/NCBI | |
|
Gong EJ and Kim DH: Endoscopic ultrasonography in the diagnosis of gastric subepithelial lesions. Clin Endosc. 49:425–433. 2016. View Article : Google Scholar : PubMed/NCBI | |
|
Nasser H, Ahmed Y, Szpunar SM and Kowalski PJ: Malignant granular cell tumor: A look into the diagnostic criteria. Pathol Res Pract. 207:164–168. 2011. View Article : Google Scholar : PubMed/NCBI | |
|
Matsumoto H, Kojima Y, Inoue T, Takegawa S, Tsuda H, Kobayashi A and Watanabe K: A malignant granular cell tumor of the stomach: Report of a case. Surg Today. 26:119–122. 1996. View Article : Google Scholar : PubMed/NCBI | |
|
Nitta T, Ohta M, Kataoka J, Ishii M, Ueda Y, Senpuku S, Takeshita A and Ishibashi T: Granular cell tumor coexisting with adenocarcinoma in the stomach: Report of a rare case. Ann Med Surg (Lond). 65:1022712021.PubMed/NCBI | |
|
Fanburg-Smith JC, Meis-Kindblom JM, Fante R and Kindblom LG: Malignant granular cell tumor of soft tissue: Diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 22:779–794. 1998. View Article : Google Scholar : PubMed/NCBI | |
|
Naidech HJ, Axelrod RS and Seliger G: Granular cell tumor (myoblastoma) of the stomach. Am J Roentgenol Radium Ther Nucl Med. 113:245–247. 1971. View Article : Google Scholar : PubMed/NCBI | |
|
Goodman MD and Cooper PH: Granular cell tumor (myoblastoma) of the stomach. A case report with ultrastructural findings and review of the literature. Am J Dig Dis. 17:1117–1126. 1972. View Article : Google Scholar : PubMed/NCBI | |
|
Miranda D: Benign granular cell tumor (‘myoblastoma’) of the stomach. Am J Gastroenterol. 65:344–348. 1976.PubMed/NCBI | |
|
Ross JS: Massive upper gastrointestinal hemorrhage from a granular cell tumor of the stomach. Am J Gastroenterol. 68:595–598. 1977.PubMed/NCBI | |
|
Chen TK: Multifocal benign granular cell tumor of the stomach. J Clin Gastroenterol. 3:65–67. 1981. View Article : Google Scholar : PubMed/NCBI | |
|
Abdelwahab IF and Klein MJ: Granular cell tumor of the stomach: A case report and review of the literature. Am J Gastroenterol. 78:71–76. 1983.PubMed/NCBI | |
|
Seo IS, Azzarelli B, Warner TF, Goheen MP and Senteney GE: Multiple visceral and cutaneous granular cell tumors ultrastructural and lmmunocytochemical evidence of schwann cell origin. Cancer. 53:2104–2110. 1984. View Article : Google Scholar : PubMed/NCBI | |
|
Shah AN and Mazza BM: Endoscopic removal of a granular cell tumor of the stomach. Gastrointest Endosc. 32:541986. View Article : Google Scholar : PubMed/NCBI | |
|
Yamaguchi K, Maeda S and Kitamura K: Granular cell tumor of the stomach coincident with two early gastric carcinomas. Am J Gastroenterol. 84:656–659. 1989.PubMed/NCBI | |
|
Joshi A, Chandrasoma P and Kiyabu M: Multiple granular cell tumors of the gastrointestinal tract with subsequent development of esophageal squamous carcinoma. Dig Dis Sci. 37:1612–1618. 1992. View Article : Google Scholar : PubMed/NCBI | |
|
Bickel A, Szvalb S, Eitan A and Cohen I: The coexistence of inflammatory fibroid polyp and cranular cell tumor in the same gastric lesion. Am J Gastroenterol. 89:2090–2091. 1994.PubMed/NCBI | |
|
White JG, eI-Newihi HM and Hauser CJ: Granular cell tumor of the stomach presenting as gastric outlet obstruction. Am J Gastroenterol. 89:2259–2260. 1994.PubMed/NCBI | |
|
Yasuda I, Tomita E, Nagura K, Nishigaki Y, Yamada O and Kachi H: Endoscopic removal of granular cell tumors. Gastrointest Endosc. 41:163–167. 1995. View Article : Google Scholar : PubMed/NCBI | |
|
David O and Jakate S: Multifocal granular cell tumor of the esophagus and proximal stomach with infiltrative pattern: A case report and review of the literature. Arch Pathol Lab Med. 123:967–973. 1999. View Article : Google Scholar : PubMed/NCBI | |
|
Eguchi S, Matsuo S, Hidaka M, Azuma T, Yamaguchi S, Hayashi T, Eguchi S and Kanematsu T: Concomitant triple lesions of adenocarcinoma, malignant lymphoma, and granular cell tumor of the stomach. J Clin Gastroenterol. 35:107–109. 2002. View Article : Google Scholar : PubMed/NCBI | |
|
Maekawa H, Maekawa T, Yabuki K, Sato K, Tamazaki Y, Kudo K, Wada R and Matsumoto M: Multiple esophagogastric granular cell tumors. J Gastroenterol. 38:776–780. 2003. View Article : Google Scholar : PubMed/NCBI | |
|
Mitomi H, Matsumoto Y, Mori A, Arai N, Ishii K, Tanabe S, Kobayashi K, Sada M and Mieno H: Multifocal granular cell tumors of the gastrointestinal tract: Immunohistochemical findings compared with those of solitary tumors. Pathol Int. 54:47–51. 2004. View Article : Google Scholar : PubMed/NCBI | |
|
Patti R, Almasio PL and Vita GD: Granular cell tumor of stomach: A case report and review of literature. World J Gastroenterol. 12:3442–3445. 2006. View Article : Google Scholar : PubMed/NCBI | |
|
Lowe DL, Chaudhary AJ, Lee JR, Chamberlain SM, Schade RR and Cuartas-Hoyos U: Four cases of patients with gastrointestinal granular cell tumors. South Med J. 100:298–300. 2007. View Article : Google Scholar : PubMed/NCBI | |
|
John BK, Dang NC, Hussain SA, Yang GC, Cham MD, Yantiss R, Joseph AS, Giashuddin SM, Lee PC, Fleming R and Somnay K: Multifocal granular cell tumor presenting as an esophageal stricture. J Gastrointest Cancer. 39:107–113. 2009. View Article : Google Scholar : PubMed/NCBI | |
|
Rekha K and Srinivas CN: Granular cell tumor of gastric mucosa. Indian J Pathol Microbiol. 53:578–579. 2010. View Article : Google Scholar : PubMed/NCBI | |
|
Pertile D, Scabini S, Romairone E, Scordamaglia R, Rimini E and Ferrando V: Gastric Abrikosoff tumor (granular cell tumor): Case report. G Chir. 31:433–434. 2010.PubMed/NCBI | |
|
Monahan KJ, Pelling M, Goldin R and Hoare J: Endoscopic removal of a granular cell tumor from the stomach using the Duette Multiband Mucosectomy kit. Dig Dis Sci. 55:2688–2690. 2009. View Article : Google Scholar : PubMed/NCBI | |
|
Gilg MM, Mrak K, Vieth M and Langner C: Granular cell tumor of the stomach. Pathologe. 33:61–64. 2012. View Article : Google Scholar : PubMed/NCBI | |
|
Krishnan A, Ramakrishnan R and Menon M: Endoscopic removal of granular cell tumors of stomach: Case report and review of literature. Gastroenterology Res. 6:240–243. 2013.PubMed/NCBI | |
|
Min KW, Lee KG, Han H, Jang SM and Paik SS: Gastric granular cell tumour clinically mimicking carcinoid tumour treated by endoscopic submucosal dissection. ANZ J Surg. 84:985–986. 2013. View Article : Google Scholar : PubMed/NCBI | |
|
Lipkin-Moore Z, Thomas RM and Rothstein RD: Multifocal synchronous granular cell tumors of the gastrointestinal tract. ACG Case Rep J. 1:193–195. 2014. View Article : Google Scholar : PubMed/NCBI | |
|
Takaya H, Kawaratani H, Kaneko M, Takeda S, Sawada Y, Kitade M, Moriya K, Namisaki T, Sawai M, Mitoro A, et al: Gastric granular cell tumor in a youth excised by endoscopic submucosal dissection: A case report and literature review. Acta Gastroenterol Belg. 80:317–319. 2017.PubMed/NCBI | |
|
Hnach Y, Allaoui M and Oukabli M: Gastric Abrikossoff tumor: about a new case. The Pan African Medical Journal. 28:2202017.(In French). PubMed/NCBI | |
|
Jain A, Karegar M, Joshi A and Rojekar A: Granular cell tumour in stomach: A case report. Indian J Surg Oncol. 9:598–600. 2018. View Article : Google Scholar : PubMed/NCBI | |
|
Watanabe Y, Watanabe M, Suehara N, Ishikawa N, Shinkawa T, Hosokawa T, Akiho H, Mine M, Tamiya S, Nishihara K and Nakano T: Early gastric cancer with diffuse heterotopic gastric glands and granular cell tumors mimicking advanced gastric cancer. Int J Surg Case Rep. 46:41–46. 2018. View Article : Google Scholar : PubMed/NCBI | |
|
Kawai M, Goda N, Nikaido M and Fukuda A: A case of gastric granular cell tumor. JGH Open. 5:966–967. 2021. View Article : Google Scholar : PubMed/NCBI | |
|
Kent T and Saulino D: Incidental multifocal granular cell tumor in the setting of chronic gastritis discovered following gastric sleeve operation: A case report and brief review of the literature. J Surg Case Rep. 2024:rjad7002024. View Article : Google Scholar : PubMed/NCBI | |
|
Abrikossoff A: Concerning myomas starting from the striated voluntary musculature. Virchows Arch Pathol Anat. 215–233. 1926.(In German). View Article : Google Scholar | |
|
Chen SY, Sadanand A, Dillon PA, He M, Dehner LP and Leonard DS: Non-Neural (S-100 Negative) bronchial granular cell tumor causing acute respiratory failure. Fetal Pediatr Pathol. 39:85–89. 2020. View Article : Google Scholar : PubMed/NCBI | |
|
Schoedel KE, Bastacky S and Silverman A: An S100 negative granular cell tumor with malignant potential: Report of a case. J Am Acad Dermatol. 39:894–898. 1998. View Article : Google Scholar : PubMed/NCBI | |
|
Mejía H, Rubiano MFO, Osorio VLD and González MI: S100 negative granular cell tumor of the oral cavity: Dermoscopy and surgical approach. An Bras Dermatol. 94:79–81. 2019. View Article : Google Scholar : PubMed/NCBI | |
|
Hirose T, Tani T, Shimada T, Ishizawa K, Shimada S and Sano T: Immunohistochemical demonstration of EMA/Glut1-positive perineurial cells and CD34-positive fibroblastic cells in peripheral nerve sheath tumors. Mod Pathol. 16:293–298. 2003. View Article : Google Scholar : PubMed/NCBI | |
|
Díaz-Flores L, Gutiérrez R, García MP, Gayoso S, Gutiérrez E, Díaz-Flores L Jr and Carrasco JL: Telocytes in the normal and pathological peripheral nervous system. Int J Mol Sci. 21:43202020. View Article : Google Scholar : PubMed/NCBI | |
|
Goto O, Kaise M and Iwakiri K: Advancements in the diagnosis of gastric subepithelial tumors. Gut Liver. 16:321–330. 2022. View Article : Google Scholar : PubMed/NCBI | |
|
Kida M, Kawaguchi Y, Miyata E, Hasegawa R, Kaneko T, Yamauchi H, Koizumi S, Okuwaki K, Miyazawa S, Iwai T, et al: Endoscopic ultrasonography diagnosis of subepithelial lesions. Dig Endosc. 29:431–443. 2017. View Article : Google Scholar : PubMed/NCBI | |
|
Pareja F, Brandes AH, Basili T, Selenica P, Geyer FC, Fan D, Da Cruz Paula A, Kumar R, Brown DN, Gularte-Mérida R, et al: Loss-of-function mutations in ATP6AP1 and ATP6AP2 in granular cell tumors. Nat Commun. 9:35332018. View Article : Google Scholar : PubMed/NCBI | |
|
Na JI, Kim HJ, Jung JJ, Kim Y, Kim SS, Lee JH, Lee KH and Park JT: Granular cell tumours of the colorectum: Histopathological and immunohistochemical evaluation of 30 cases. Histopathology. 65:764–774. 2014. View Article : Google Scholar : PubMed/NCBI | |
|
Murakata LA and Ishak KG: Expression of inhibin-alpha by granular cell tumors of the gallbladder and extrahepatic bile ducts. Am J Surg Pathol. 25:1200–1203. 2001. View Article : Google Scholar : PubMed/NCBI | |
|
Stenvers KL and Findlay JK: Inhibins: From reproductive hormones to tumor suppressors. Trends Endocrinol Metab. 21:174–180. 2010. View Article : Google Scholar : PubMed/NCBI | |
|
Weidemann S, Noori NA, Lennartz M, Lennartz M, Reiswich V, Dum D, Menz A, Chirico V, Hube-Magg C, Fraune C, et al: Inhibin alpha expression in human tumors: A tissue microarray study on 12,212 tumors. Biomedicines. 10:25072022. View Article : Google Scholar : PubMed/NCBI | |
|
Ortiz-Hidalgo C and Frías-Soria CL: Análisis histopatológico e inmunohistoquímico del tumor de células granulares. Estudios de 12 casos con una breve nota histórica. Rev Esp Patol. 52:11–19. 2019.(In Spanish). PubMed/NCBI | |
|
Le BH, Boyer PJ, Lewis JE and Kapadia SB: Granular cell tumor: Immunohistochemical assessment of inhibin-alpha, protein gene product 9.5, S100 protein, CD68, and Ki-67 proliferative index with clinical correlation. Arch Pathol Lab Med. 128:771–775. 2004. View Article : Google Scholar : PubMed/NCBI | |
|
Fine SW and Li M: Expression of calretinin and the alpha-subunit of inhibin in granular cell tumors. Am J Clin Pathol. 119:259–264. 2003. View Article : Google Scholar : PubMed/NCBI | |
|
Doyle LA, Hornick JL and Fletcher CDM: PEComa of the gastrointestinal tract clinicopathologic study of 35 cases with evaluation of prognostic parameters. Am J Surg Pathol. 37:1769–1782. 2013. View Article : Google Scholar : PubMed/NCBI | |
|
Lauricella S, Valeri S, Mascianà G, Gallo IF, Mazzotta E, Pagnoni C, Costanza S, Falcone L, Benvenuto D, Caricato M and Capolupo GT: What about gastric Schwannoma? A review article. J Gastrointest Cancer. 52:57–67. 2020. View Article : Google Scholar | |
|
Papke DJ and Hornick JL: Recent developments in gastroesophageal mesenchymal tumours. Histopathology. 78:171–186. 2020. View Article : Google Scholar : PubMed/NCBI | |
|
Machado I, Cruz J, Lavernia J and Llombart-Bosch A: Solitary, multiple, benign, atypical, or malignant: The ‘Granular Cell Tumor’ puzzle. Virchows Arch. 468:527–538. 2015. View Article : Google Scholar : PubMed/NCBI | |
|
Deprez PH, Moons LMG, O'Toole D, Gincul R, Seicean A, Pimentel-Nunes P, Fernández-Esparrach G, Polkowski M, Vieth M, Borbath I, et al: Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European society of gastrointestinal endoscopy (ESGE) guideline. Endoscopy. 54:412–429. 2022. View Article : Google Scholar : PubMed/NCBI | |
|
Barakata M, Kar AA, Pourshahid S, Ainechi S, Lee HJ, Othman M and Tadros M: Gastrointestinal and biliary granular cell tumor: Diagnosis and management. Ann Gastroenterol. 31:439–447. 2018.PubMed/NCBI | |
|
Ryu DG, Choi CW, Kim SJ, Hwang CS, Kang DH, Kim HW, Park SB and Son BS: Clinical outcomes of esophageal granular cell tumors with different endoscopic resection methods. Sci Rep. 13:107382023. View Article : Google Scholar : PubMed/NCBI | |
|
Tada M, Karita M, Yanai H and Takemoto T: Endoscopic therapy of early gastric cancer by strip biopsy. Gan To Kagaku Ryoho. 15:1460–1465. 1988.(In Japanese). PubMed/NCBI | |
|
Maple JT, Dayyeh BK, Chauhan SS, Hwang JH, Komanduri S, Manfredi M, Konda V, Murad FM, Siddiqui UD and Banerjee S: Endoscopic submucosal dissection. Gastrointest Endosc. 81:1311–1325. 2015. View Article : Google Scholar : PubMed/NCBI | |
|
Kahng DH, Kim GH, Park DY, Jeon MS, Yi JW, Choi YY and Song GA: Endoscopic resection of granular cell tumors in the gastrointestinal tract: A single center experience. Surg Endosc. 27:3228–3236. 2013. View Article : Google Scholar : PubMed/NCBI |









