



Aged garlic extract reduces low attenuation plaque in coronary arteries of patients with diabetes: A randomized, double‑blind, placebo‑controlled study
- Authors:
- Published online on: December 27, 2019 https://doi.org/10.3892/etm.2019.8371
- Pages: 1457-1461
-
Copyright: © Shaikh et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
Introduction
Coronary artery disease (CAD) is the leading cause of morbidity and mortality in individuals with diabetes. According to the report of the American Diabetes Association (ADA), the estimated cost related to the treatment of cardiovascular event is $37.3 billion annually in individuals with diabetes in the US alone (1). Unfortunately, however, the incidence of diabetes is increasing in epidemic proportions worldwide. It is estimated 170 million individuals are living with diabetes worldwide and its prevalence is estimated to double by 2030 (2). A previous study demonstrated that the risk of mortality from cardiovascular causes in subjects with type 2 diabetes mellitus (T2DM) and no previous history of cardiovascular events is equivalent to that of non-DM subjects with prior myocardial infarction (MI) (3). Asymptomatic atherosclerosis has usually been present for years and even decades prior to the development of clinical evidence of CAD (4,5). Screening for the early detection of patients who are at risk of developing asymptomatic atherosclerosis and monitoring their response to treatment in order to reduce cardiovascular events remains a major challenge in preventive cardiology. Coronary computed tomography angiography (CCTA) is considered a reliable tool with which to detect or rule out the presence, extent and severity of coronary atherosclerosis (6).
Previous studies demonstrated that statin and anti-diabetic therapies may decrease the rate of coronary plaque progression and may participate in plaque stabilization (7–9). Previous experiments performed in our laboratory have shown that the use of aged garlic extract (AGE) is associated with a significant reduction in low attenuation plaque (LAP) progression as compared to the placebo using CCTA in patients with metabolic syndrome (10). Furthermore, AGE has been shown to exert positive effects on several cardiovascular disease risk factors, including endothelial dysfunction, cholesterol and blood pressure (11–14). The aim of the present study was to evaluate the effects of AGE over a period of 1 year on coronary atherosclerotic plaque in individuals with T2DM utilizing CCTA.
Patients and methods
Study design
This study was a single-center, randomized, placebo-controlled, double-blind trial being conducted at the Lundquist Institute for Biomedical Innovation at Harbor UCLA Medical Center. In total, 80 individuals, who met the eligibility criteria (inclusion and exclusion criteria) were enrolled in this study. After signing a written informed consent, cardiovascular risk factors and blood samples were collected following a 12-h fast. Sample were stored at −70°C and analyzed for hemoglobin A1c (HbA1c) levels and lipid profiles, including serum low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol and triglycerides (TGs), with the use of automated diagnostic equipment (DLS Laboratories). All participants underwent CAC scanning and CCTA to evaluate early CAD. Patients were randomized at a 1:1 ratio to receive 2,400 mg AGE/day or a placebo. The intended duration of administration for the study group was 12 months. This study was approved by the Institutional Review Board of Lundquist Institute for Biomedical Innovation at Harbor UCLA Medical Center (Clinicaltrials.gov: NCT03931434).
Inclusion criteria
Patients with T2DM were enrolled in this study. The age of the patients was between 30–75 years and the patients had HbA1c levels >6.5% or fasting blood sugar levels >125 mg/dl, or were taking anti-diabetic medications and who provided the written informed consent.
Exclusion criteria
Individuals with known hypersensitivity to AGE, a body weight >300 lbs, a history of bleeding disorders or those taking anti-coagulants, those with hypertensive encephalopathy or cerebrovascular event, a known history of CAD, MI, stroke or life-threatening arrhythmia within the prior 6 months, New York Heart Association Functional Classification II–IV heart failure, renal impairment (serum creatinine levels, >1.4 mg/dl), current tobacco use, or who were currently enrolled in another placebo-controlled trial or females with pregnancy were excluded.
Outcome measures
The outcome measures included the rate of change in coronary plaque volume and vulnerable component of coronary plaques.
AGE
AGE (Kyolic) is formulated by soaking sliced raw garlic in aqueous ethanol solution at room temperature for up to 20 months as previously described (11,12). The 2,400 mg of AGE capsules were provided by Wakunaga of America Co., Ltd. with a matched placebo pill. The placebo and the study drug appeared to be of similar size and color; however, the placebo pill did not contain any garlic or active ingredient. All participants were advised to take 2 capsules twice daily with water for 12 months. An inter-trial phone visit was conducted to ensure study medication compliance. The AGE capsule used in this study is commercially available in the market.
Data acquisition
The details of coronary artery plaque volume by CCTA assessment have been published in previous studies (6,15). Non-contrast scans for the evaluation of the extent of coronary artery calcium and contrast scans for the evaluation of coronary artery plaque volume at baseline and 12 months were acquired. Scans were assessed by readers who were blinded both to treatment group and to the date of the scan.
Coronary plaque assessment
Quantitative plaque assessment was performed according to a previously defined protocol (10) using semi-automated plaque analysis software (QAngioCT Research Edition Version 2.0.5; Medis Medical Imaging Systems). Based on the guidelines of the Society of Cardiovascular Computed Tomography, 17-segment coronary artery model vessels based on SCCT guidelines were assessed. Only vessels >1.5 mm were evaluated. The volumes of 4 types of coronary artery plaque [LAP, fibro-fatty (FF), fibrous (F) and dense calcium (DC)] were calculated using the Hounsfield unit threshold.
Statistical analyses
Continuous variables are expressed as the means ± standard deviation (SD), while categorical variables are stated as counts and percentages. A Student's t-test or Chi-square test was used to assess differences in all baseline parameters between the placebo and AGE. The analysis included comparisons for both plaque levels at both baseline and follow-up and between groups following the use of the ANOVA modeling with the Tukey approach P-value. ANCOVA modeling was also used to adjust for clinically significant variables. As none of these modeling techniques were significant, we thus chose to focus on the simple progression of LAP in the placebo group and regression in the active group. Atherosclerotic plaque volumes differences between the placebo and AGE were assessed by the Wilcoxon rank-sum test. A P-value <0.05 was considered to indicate a statistically significant difference. SAS software (version 9.4) was used to carry out all statistical analyses.
Results
From 2016 to 2017, 80 patients were enrolled and randomly assigned to the placebo or AGE groups. In total, 66 patients completed the study with baseline and follow-up CT. The participants had a mean follow-up period of 370±24 days. Of these patients, 28% in the placebo group and 29% in the active group were on statins. Patients in both groups continued to see their primary care physicians and continued their regular medications. All the baseline data at entry into this study in both groups have been previously described (16). No statistically significant differences were found between the groups.
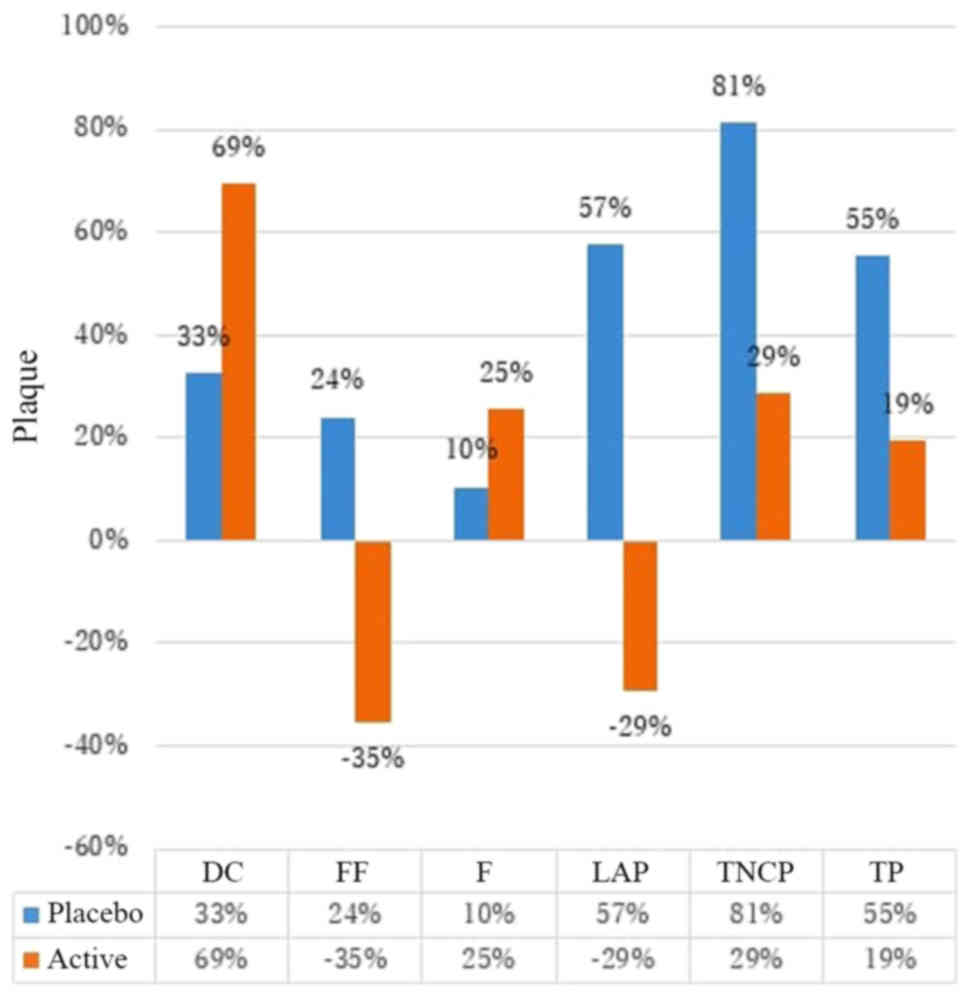
The AGE group compared with the placebo group exhibited a statistically significant regression in normalized LAP [median SD) −0.2 (18.8) vs. 2.5 (69.3), P=0.0415]. By percentage, there was 29% reduction in LAP in the AGE group as opposed to 57% LAP plaque progression in the placebo group. The AGE group exhibited a reduction in FF plaque as compared to the progression of FF in the placebo group; however this did not reach statistically significance (median difference −0.1 vs. +1.6, P-0.287). No marked differences were observed in total plaque (TP), F, or FF plaque volumes between the AGE and placebo group (Table I and Fig. 1).
Discussion
In this study, 1 year of AGE therapy was associated with a regression of LAP. LAP [non-calcified plaque (NCP) <30 HU] is one of the high-risk plaque features. The results of this study are in concordance with those of previously published studies demonstrating the regression of LAP in participants with metabolic syndrome and general population in studies of AGE (10,17), as well as statin studies (18,19).
According to certain data, LAP represents an intravascular ultrasound (IVUS) equivalent of the necrotic core (19). In contrast to more stable F plaques, plaques with a lipid-rich necrotic core play a significant role in the development of acute coronary syndrome (ACS) (20). Recent advancements in cardiac imaging modalities have provided an accurate and detailed quantitative assessment of plaque composition and burden based on differences in CCTA (21). Previous studies have demonstrated an increased risk of myocardial infarction and cardiovascular death in patients with a larger volume of non-calcified and low-attenuation plaque (22,23).
Motoyama et al (24) demonstrated that patients with ACS exhibited a significantly increased frequency of low attenuation plaque (79 vs. 9%, P<0.001). Balestrieri et al (9) reported that the patients with stable chest pain with adverse plaque features, including LAP, spotty calcification and positive remodeling found an association with a 60% increased risk of future adverse cardiovascular events. Furthermore, LAP along with other vulnerable plaque features have been shown to be associated with rapidly progressive CAD (25). The SCOT-HEART trial, which consisted of mostly intermediate risk patients, demonstrated that low attenuation was associated with a 3-fold increased risk of non-fatal MI or coronary heart disease-associated mortality (26). In this study, there was a 57% increase in low attenuation plaque in the placebo group, representing the natural history of plaque progression. By contrast, a 29% reduction was observed in LAP in the AGE group over a period of 1-year follow-up, strongly suggesting the therapeutic potential of AGE in the diabetic population (Fig. 1).
The present study has several limitations. First, this relatively small sample size and short-term follow-up study did not have enough power to demonstrate the significant differences in TP volume, NCP and DC. Second, patients were under different therapies for hyperlipidemia and T2DM, and some patients used varying medications at different doses. Due to the small sample size, a separate analysis with different hyperlipidemia and T2DM medications was not performed. Further research is thus required to evaluate whether AGE has the ability to stabilize vulnerable plaque and to decrease adverse cardiovascular events.
Acknowledgements
Not applicable.
Funding
This study was funded by Wakunaga of America Co., Ltd., Mission Viejo, CA, USA.
Availability of data and materials
All data generated or analyzed during this study are included in this published article or are available from the corresponding author on reasonable request.
Authors' contributions
MJB conceived of and designed the study. KS, LC, DB, RN, SA, EJ, CS, FF, SH, MSH, AJ, BC and MJB collected the patient information and generated the clinical data. AK, KS, LC, DB, RN, SA and MJB analyzed and/or interpreted the data; and KS, AK, LC, RN and MJB drafted or revised the manuscript. All authors have read and approved the final version of the manuscript.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Lundquist Institute for Biomedical Innovation at Harbor UCLA Medical Center (Clinicaltrials.gov: NCT03931434). All patients provided signed and written informed consent.
Patient consent for publication
Not applicable.
Competing interests
MJB discloses work for the National Institutes of Health and General Electric Healthcare. All the other authors declare that they have no competing interests.
References
|
American Diabetes Association, . 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2019. Diabetes Care. 42 (Suppl 1):S103–S123. 2019. View Article : Google Scholar : PubMed/NCBI | |
|
Wild S, Roglic G, Green A, Sicree R and King H: Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 27:1047–1053. 2004. View Article : Google Scholar : PubMed/NCBI | |
|
Haffner SM, Lehto S, Rönnemaa T, Pyörälä K and Laakso M: Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 339:229–234. 1998. View Article : Google Scholar : PubMed/NCBI | |
|
Eggen DA, Strong JP and McGill HC Jr: Coronary calcification. Relationship to clinically significant coronary lesions and race, sex, and topographic distribution. Circulation. 32:948–955. 1965. View Article : Google Scholar : PubMed/NCBI | |
|
Burchfiel CM, Reed DM, Marcus EB, Strong JP and Hayashi T: Association of diabetes mellitus with coronary atherosclerosis and myocardial lesions. An autopsy study from the Honolulu Heart Program. Am J Epidemiol. 137:1328–1340. 1993. View Article : Google Scholar : PubMed/NCBI | |
|
Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, Scherer M, Bellinger R, Martin A, Benton R, et al: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 52:1724–1732. 2008. View Article : Google Scholar : PubMed/NCBI | |
|
Schartl M, Bocksch W, Koschyk DH, Voelker W, Karsch KR, Kreuzer J, Hausmann D, Beckmann S and Gross M: Use of intravascular ultrasound to compare effects of different strategies of lipid-lowering therapy on plaque volume and composition in patients with coronary artery disease. Circulation. 104:387–392. 2001. View Article : Google Scholar : PubMed/NCBI | |
|
Tian Y, Chen T, Wu Y, Yang L, Wang L, Fan X, Zhang W, Feng J, Yu H, Yang Y, et al: Pioglitazone stabilizes atherosclerotic plaque by regulating the Th17/Treg balance in AMPK-dependent mechanisms. Cardiovasc Diabetol. 16:1402017. View Article : Google Scholar : PubMed/NCBI | |
|
Balestrieri ML, Rizzo MR, Barbieri M, Paolisso P, D'Onofrio N, Giovane A, Siniscalchi M, Minicucci F, Sardu C, D'Andrea D, et al: Sirtuin 6 expression and inflammatory activity in diabetic atherosclerotic plaques: Effects of incretin treatment. Diabetes. 64:1395–1406. 2015. View Article : Google Scholar : PubMed/NCBI | |
|
Matsumoto S, Nakanishi R, Li D, Alani A, Rezaeian P, Prabhu S, Abraham J, Fahmy MA, Dailing C, Flores F, et al: Aged Garlic Extract Reduces Low Attenuation Plaque in Coronary Arteries of Patients with Metabolic Syndrome in a Prospective Randomized Double-Blind Study. J Nutr. 146:427S–432S. 2016. View Article : Google Scholar : PubMed/NCBI | |
|
Budoff MJ, Takasu J, Flores FR, Niihara Y, Lu B, Lau BH, Rosen RT and Amagase H: Inhibiting progression of coronary calcification using Aged Garlic Extract in patients receiving statin therapy: A preliminary study. Prev Med. 39:985–991. 2004. View Article : Google Scholar : PubMed/NCBI | |
|
Budoff MJ, Ahmadi N, Gul KM, Liu ST, Flores FR, Tiano J, Takasu J, Miller E and Tsimikas S: Aged garlic extract supplemented with B vitamins, folic acid and L-arginine retards the progression of subclinical atherosclerosis: A randomized clinical trial. Prev Med. 49:101–107. 2009. View Article : Google Scholar : PubMed/NCBI | |
|
Larijani VN, Ahmadi N, Zeb I, Khan F, Flores F and Budoff M: Beneficial effects of aged garlic extract and coenzyme Q10 on vascular elasticity and endothelial function: The FAITH randomized clinical trial. Nutrition. 29:71–75. 2013. View Article : Google Scholar : PubMed/NCBI | |
|
Ried K and Fakler P: Potential of garlic (Allium sativum) in lowering high blood pressure: Mechanisms of action and clinical relevance. Integr Blood Press Control. 7:71–82. 2014. View Article : Google Scholar : PubMed/NCBI | |
|
Mao SS, Li D, Rosenthal DG, Cerilles M, Zeb I, Wu H, Flores F, Gao Y and Budoff MJ: Dual-standard reference values of left ventricular volumetric parameters by multidetector CT angiography. J Cardiovasc Comput Tomogr. 7:234–240. 2013. View Article : Google Scholar : PubMed/NCBI | |
|
Hutchins E, Shaikh K, Kinninger A, et al: Aged garlic extract may reduce left ventricular myocardial mass in patients with diabetes: A prospective randomized controlled double-blind study. Exp Ther Med (In press). | |
|
Zeb I, Ahmadi N, Nasir K, Kadakia J, Larijani VN, Flores F, Li D and Budoff MJ: Aged garlic extract and coenzyme Q10 have favorable effect on inflammatory markers and coronary atherosclerosis progression: A randomized clinical trial. J Cardiovasc Dis Res. 3:185–190. 2012. View Article : Google Scholar : PubMed/NCBI | |
|
Zeb I, Li D, Nasir K, Malpeso J, Batool A, Flores F, Dailing C, Karlsberg RP and Budoff M: Effect of statin treatment on coronary plaque progression - a serial coronary CT angiography study. Atherosclerosis. 231:198–204. 2013. View Article : Google Scholar : PubMed/NCBI | |
|
Nakanishi R, Alani A, Matsumoto S, Li D, Fahmy M, Abraham J, Dailing C, Broersen A, Kitslaar PH, Nasir K, et al: Changes in coronary plaque volume: Comparison of serial measurements on intravascular ultrasound and coronary computed tomographic angiography. Tex Heart Inst J. 45:84–91. 2018. View Article : Google Scholar : PubMed/NCBI | |
|
Ihdayhid AR, Goeller M, Dey D, Nerlekar N, Yap G, Thakur U, Adams D, Cameron J, Seneviratne S, Achenbach S, et al: Comparison of Coronary Atherosclerotic Plaque Burden and Composition as Assessed on Coronary Computed Tomography Angiography in East Asian and European-Origin Caucasians. Am J Cardiol. 124:1012–1019. 2019. View Article : Google Scholar : PubMed/NCBI | |
|
Voros S, Rinehart S, Qian Z, Vazquez G, Anderson H, Murrieta L, Wilmer C, Carlson H, Taylor K, Ballard W, et al: Prospective validation of standardized, 3-dimensional, quantitative coronary computed tomographic plaque measurements using radiofrequency backscatter intravascular ultrasound as reference standard in intermediate coronary arterial lesions: Results from the ATLANTA (assessment of tissue characteristics, lesion morphology, and hemodynamics by angiography with fractional flow reserve, intravascular ultrasound and virtual histology, and noninvasive computed tomography in atherosclerotic plaques) I study. JACC Cardiovasc Interv. 4:198–208. 2011. View Article : Google Scholar : PubMed/NCBI | |
|
Versteylen MO, Kietselaer BL, Dagnelie PC, Joosen IA, Dedic A, Raaijmakers RH, Wildberger JE, Nieman K, Crijns HJ, Niessen WJ, et al: Additive value of semiautomated quantification of coronary artery disease using cardiac computed tomographic angiography to predict future acute coronary syndrome. J Am Coll Cardiol. 61:2296–2305. 2013. View Article : Google Scholar : PubMed/NCBI | |
|
Hell MM, Motwani M, Otaki Y, Cadet S, Gransar H, Miranda-Peats R, Valk J, Slomka PJ, Cheng VY, Rozanski A, et al: Quantitative global plaque characteristics from coronary computed tomography angiography for the prediction of future cardiac mortality during long-term follow-up. Eur Heart J Cardiovasc Imaging. 18:1331–1339. 2017. View Article : Google Scholar : PubMed/NCBI | |
|
Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T, Naruse H, Ishii J, Hishida H, Wong ND, et al: Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol. 54:49–57. 2009. View Article : Google Scholar : PubMed/NCBI | |
|
Chang H-J, Lin FY, Lee S-E, Andreini D, Bax J, Cademartiri F, Chinnaiyan K, Chow BJW, Conte E, Cury RC, et al: Coronary atherosclerotic precursors of acute coronary syndromes. J Am Coll Cardiol. 71:2511–2522. 2018. View Article : Google Scholar : PubMed/NCBI | |
|
Williams MC, Moss AJ, Dweck M, Adamson PD, Alam S, Hunter A, Shah ASV, Pawade T, Weir-McCall JR, Roditi G, et al: Coronary Artery Plaque Characteristics Associated With Adverse Outcomes in the SCOT-HEART Study. J Am Coll Cardiol. 73:291–301. 2019. View Article : Google Scholar : PubMed/NCBI |









