



Focusing on colorectal cancer in young adults (Review)
- Authors:
- Published online on: December 6, 2023 https://doi.org/10.3892/mco.2023.2706
- Article Number: 8
-
Copyright: © Constantinou et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
1. Introduction
Colorectal cancer (CRC) which comprises cancer of the colon and/or rectum, is the third most common cancer worldwide, with more than 1.93 million new cases and 935,173 deaths reported globally in the year 2020(1). CRC ranks third in cancer-associated mortality in both males and females worldwide, and its incidence has uniquely increased in various high-income countries, including the United States, Germany, the United Kingdom, Australia, and Canada (2,3).
In the mid-1990s, screening for CRC begun among average-risk individuals across the population for all adults who were 50 years of age and above. Since then, the incidence and subsequently the mortality for ‘late onset CRC (loCRC)’ among individuals 50 years or older have been decreasing (4). On the contrary, the incidence of CRC in young adults under 50 years old, defined as early-onset CRC has dramatically increased since the mid-1990s (2). In this article, the term ‘late-onset CRC (loCRC)’ will refer to individuals 50 years or older, and ‘early-onset CRC (eoCRC)’ will refer to patients diagnosed with CRC before the age of 50. Currently, the largest percentage of people suffering from eoCRC falls within the 40-49 age group, accounting for approximately one in eight new cases of CRC (5) and comprising an overall 10-12% of total CRC diagnoses (6).
CRC develops when stem cells resigning at the base of the colon crypts undergo genetic and epigenetic modifications which affect oncogenes and tumour suppressor genes, leading to the transformation of normal stem cells to cancerous stem cells (7). Through multiple rounds of clonal expansion of selected cells, colon cells undergo malignant transformation, resulting in loss of genomic stability (8).
The majority of CRC cases occur sporadically (94%) with main precursors involving an adenoma or serrated lesion, while the minority (5%) are the result of inherited predisposition syndromes, including the Lynch Syndrome and the Familial Adenomatous Polyposis (FAP) syndromes, and with only 1% being attributed to chronic inflammatory conditions (9).
Colon tumours are located in the proximal colon, encompassing the cecum and the ascending and transverse colon, and in the distal colon, encompassing the descending and sigmoid colon. Rectal tumours are located in the rectosigmoid junction and rectum. There is variation in the anatomical dispersion of CRC due to age and sex; for example, the frequency of cancer diagnosis in the distal colon and rectum is higher in the younger population group (adults between 18-49) compared to the frequency reported in the older population group (adults older than 50 years) (10).
The younger individuals suffering from eoCRC have differences both in their clinical presentation as well as their tumour histology when compared to older individuals suffering from loCRC (11). A higher recurrence of advanced disease and more invasive features are reported in younger individuals, signifying the urgent need to understand the possible aetiologies behind these trends (12,13). Patients under the age of 50 commonly present with a later stage of cancer due to a delay in diagnosis (14-16). One study has supported that the time lapse from the initiation of symptoms to consultation with a primary care provider may be 6-fold longer in younger patients than in older patients (17). Young adults may also have greater odds of a second primary malignancy in the initial 6-11 months after a CRC diagnosis, compared to older patients who have reduced rates, possibly due to specific risk factors contributing to the pathogenesis of eoCRC (18). In addition to age and family history of CRC, well-documented modifiable risk factors of eoCRC include obesity, type II diabetes, unhealthy diet, physical inactivity, and frequent antibiotic use (19).
Colonoscopy represents a truly preventative CRC screening measure since it detects adenocarcinoma formation and, therefore, prevents progression towards malignancy (20). In older individuals, around 65% of the population at risk is regularly screened, and incidence has significantly dropped for the age group 50-65 by 0.7% and by 4% in individuals above 65 years of age from 2007 to 2016(4). On the other hand, the increased incidence of eoCRC could be attributed to unavailability of screening, and evidence has shown that approximately 25% of eoCRC cases could have been averted through awareness of positive family history being a risk factor and prompt commencement of screening in high-risk individuals (21).
Evidence is now emerging regarding the drivers of sporadic onset of eoCRC; yet it remains unclear whether these individuals present with distinct clinical features and pathways involved in carcinogenesis. Moreover, it remains to be elucidated whether certain environmental triggers and sedentary lifestyle are key contributors to the rising incidence in young adults. Despite similar treatment options in CRC patients regardless of age, comprehending the molecular mechanisms of eoCRC will aid in improving approaches in treatment and prevention (22).
Guidelines with regards to the treatment of eoCRC do not distinguish among younger and older patients; yet evidence supports that younger patients may receive more intensive treatment (23), while clinical outcomes and response to chemotherapy may be similar across age groups (16).
The aim of this paper is to provide an overview of our current knowledge on CRC with a focus on epidemiology, presentation, pathophysiology, and prevention of disease among young individuals.
2. Methods
The databases used to retrieve articles to be included in this narrative review were PubMed, EBSCO and Cochrane Library. We employed the following search terms: ‘colorectal cancer’, ‘incidence’, ‘early-age onset’, ‘young adults’, ‘sporadic’, ‘mortality’, ‘epidemiology’, ‘developed countries’, ‘risk factors’, ‘obesity’, ‘screening guidelines’. The selected articles were within the timeframe of 20091 to 2023, and we exclusively included journal articles published in the English language. Additional information was retrieved from the American Cancer Society, WHO and NICE guidelines. The clinical trials were retrieved from Clinicaltrials.gov using the keywords: ‘gene mutations’, ‘early age’, ‘genetic analysis’.
3. Epidemiology
Incidence and prevalence
CRC is the third most commonly diagnosed cancer worldwide among both sexes, accounting for 10% of global cancer incidence. According to GLOBOCAN 2020, there were 1.15 million new colon cancer cases, 0.7 million new rectal cancer cases and 50,000 new anal cancer cases in the year 2020 worldwide (1). The age standardized incidence rates across the world were 23.4 in males and 16.2 in females per 100,000 population in the year 2020 indicating a slight predominance in males (44% higher incidence in males vs. females) (1).
Globally over 1.93 million new cases of CRC patients were reported for the year 2020(1), of which 17,930 new cases were individuals younger than 50 years of age (4). The estimated worldwide incidence of eoCRC in 2020 revealed that it was the fourth most common cancer (24). Currently, it is expected that 1 in 23 men (4.4%) and 1 in 25 women (4.1%) in the US will have a CRC diagnosis in the course of their lives (4).
In 2019, the average global incidence rate of eoCRC was 5.7 (per 100,000 person-years), with males having a 6.9 incidence rate (per 100,000 person-years) and females having a 4.6 incidence rate (per 100,000 person-years), also indicating a slight male predominance in individuals with eoCRC (2.3 higher incidence rate in males vs. females) (25).
Generally, a rise in incidence has been reported in low-income and middle-income countries, while it has been declining or stabilizing in high-income countries that implement screening for individuals above 50 years of age (26). Contrary to the decline in incidence patterns from 2014 to 2018, with a decrease of approximately 2% per year in those aged 50 and older, the incidence of CRC in younger adults for the same period has risen by 1.5% per year (27). Japan, China and the USA are the top three countries with the highest incidence of CRC (1). The steepest rises in incidence rates from a 47-state cancer registry are in non-Hispanic whites in most states in the USA (3). An increase in the incidence of CRC in young adults has also been observed in other high-income countries, including Australia, the United Kingdom, Canada, and Germany (3). Age-standardized incidence rates of Hungary, Slovakia and Norway were the highest in 2020, with rates of 45.3, 43.9 and 41.9 per 100,000 persons, respectively (1). In the years 2012 to 2016, the incidence rates varied from 30 (per 100,000 persons) in Asia/Pacific Islanders to 45.7 (per 100,000 persons) in non-Hispanic black individuals and 43.3 (per 100,000 persons) in American Indian/Alaskan natives (4). Data from the National Cancer Institute in the USA indicate that for the time period 2006-2016, in all five-year age groups from 20-49, the steepest rise was among the group of 40-49 years of age (23). The National Comprehensive Cancer Network guidelines estimated that the rate of incidence of colon and rectal cancers will rise by 90 and 124.2%, respectively, for patients of 20-34 years of age by the year 2023(28).
Mortality and survival rates
Analogous to the incidence patterns, the mortality rate of CRC varies in different age groups with steady annual decline in the elderly and a steady annual increase in those younger than 50 years, as reported in recent years. According to data from GLOBOCAN 2020, the highest mortality of CRC in 2020 for both sexes was in Asia (54.2%), followed by Europe (26.2%), Latin America and the Caribbean (7.4%), and the lowest in Africa with 4.6% (29).
The CRC mortality rates in the US for the time period of 2008-2017 decreased by 3% per year in those older than 65 years and by 0.6% per year in those aged 50-64 years. On the contrary, for individuals younger than 50 years, the mortality rate increased by 1.3% (4). The global death rate in eoCRC increased from 1.9 per 100,000 people in 1990 to 2.2 per 100,000 people in 2019, with the highest death rates per 100,000 person-years in Seychelles, Bulgaria and Ukraine (25).
Major advancements in treating CRC, such as the removal of polyps and improved screening efforts, have contributed to high five-year survival rates at initial stages of diagnosis. For the period of 2010-2014, the 5-year net survival in most countries in western Europe and North America was between 60 and 70%, while in Africa, Asia, South America, and Eastern Europe, it was less than 50% (30). In the USA, in the years 2008-2014, the five-year relative survival rates were 92% for stage I colon cancer, 87% for stage IIA, and 65% for stage IIB. Surprisingly, the 5-year survival rates were slightly higher for stage III when compared to stage II, i.e., the survival rate was 90% for stage IIIA and 72% for stage IIIB, 53% for Stage IIIC and 12% for stage IV (metastasis) (31). The 5-year relative survival rate for people diagnosed with colon cancer between 2012 and 2018 was 91% for localized SEER stage, 72% for regional, and 13% for distant stage. For people diagnosed with rectal cancer in the same time period, the 5-year relative survival rate was 90% for localized, 74% for regional, and 17% for distant stage (32).
Risk factors
Despite a greater fraction of early CRCs being hereditary, the majority of CRCs cases are sporadic (4).
Non-modifiable risk factors
The main non-modifiable risk factor for CRC is family history, as individuals with a first-degree relative with CRC have a two to four times higher risk of being diagnosed with the disease before 50 years old and have several affected family members. Particular under-recognition of inherited colon cancer conditions like Lynch syndrome and FAP exists, contributing s to the rise in the incidence rates. For instance, in patients diagnosed with CRC from 1990 to 2010 under the age of 50, only 27% undertook genetic screening testing for Lynch Syndrome (5).
Modifiable risk factors
While the mechanisms underlying the established increase in the incidence of sporadic CRC in young adults remain unresolved, several modifiable risk factors, namely obesity, type II diabetes, antibiotic use, diet, and physical activity are implicated in the pathogenesis of eoCRC (20).
Obesity. Insulin resistance, hyperinsulinemia, and increased inflammation are associated with weight gain in early adulthood (at 18 years of age) and an increased BMI, linking obesity, as well as diabetes and sedentary lifestyle, to eoCRC (33).
In a study among 85,256 nurses aged 25-42 years, it was discovered that for every 5-unit rise in Body Mass Index (BMI), there was a 20% higher risk of early-onset CRC driven sporadically, and that both weight gain starting from 18 years of age and BMI at 18 promoted this association. Those with a BMI≥30 had almost double the risk of eoCRC in comparison to those with BMI at 18.5-22.9(33).
Nutrition. A positive association has been reported between increased CRC incidence and excess consumption of red and processed meat (34). Evidence has suggested that antibiotic use, with potential alterations in the constitution of the gut microbiome, is also correlated to increased CRC risk. Increased duration of antibiotic use in age groups 20-39 and 40-59 was significantly related to an elevated likelihood of colorectal adenoma which is the precursor for most CRCs (35).
Gut microbiota. Modifications in the gut microbiome from obesity, antibiotic use, and consumption of red and processed meats found in Western diet lead to intestinal dysbiosis. Some bacteria (proteobacteria and fusobacteria) are pro-tumourigenic and cause alterations in colon integrity, thereby having a direct effect on inflammatory responses via the production of toxins, short chain fatty acids, and changes in the composition of bile acid (34).
4. Disease presentation
The most common symptoms of CRC include rectal bleeding, abdominal pain, change in bowel habits and anaemia (36). In addition, haematochezia and abdominal pain have been reported as the most common symptoms at presentation in young patients less than 50 years of age when compared to patients older than 50 (Haematochezia: 28.8% in <50 vs. 23.2% in >50 and Abdominal pain: 41.2% in <50 vs. 27.2% in >50) (15).
An increased incidence of CRC in younger patients has been associated with left-sided cancer, which can emerge with a change in bowel habits because of bowel lumen narrowing. It can usually manifest with diarrhoea, change in stool form and subsequently bowel obstruction. Nevertheless, the symptoms are also typical of other disorders contributing to serious delays in diagnosis. In comparison to older cohorts, most young patients suffering from CRC present with a more advanced stage of disease and poorer tumour differentiation. Abdominal distension, vomiting and weight loss are indicative of advanced disease and rectal pain may flag up a bulky tumour with local pelvic invasion. Metastatic disease has been reported in 61.2% of young patients in comparison to 44.5% in those above 50, and there may be evident hepatomegaly or a palpable abdominal mass (37).
5. Diagnosis
Patient and family history
Patient consultations provide the opportunity for doctors to inquire about their patients' personal and family history. It is important for doctors to obtain a thorough family history that spans three generations. Constructing a family pedigree allows for a visual representation of family cancers, and this structure can be easily updated as new information becomes available (38).
In the presence of any possible symptoms, general practitioners (GPs) should ask if the patient has a family history of CRC or whether they have a predisposing condition, such as FAP. Specifically, GPs must collect information regarding the degree of kinship, the number of relatives diagnosed with CRC, and the age of affected individuals among those who have biological relatives with a history of either CRC or colorectal adenomas (39). However, it is important to note that doctors should be reminded that young adults with eoCRC may not exhibit evident risk factors, such as family history, which could guide early diagnosis of the disease (6).
Clinical examination
In cases where colon cancer is suspected, during a clinical consultation, doctors focus on clinical examination and laboratory findings. A major contribution to the diagnosis of CRC in almost one-third of the patients is abdominal examination. A digital examination is of equal diagnostic importance and more applicable for rectal compared to colon cancer patients (40).
Non-invasive tests and blood tests
Primary non-invasive screening tools include guaiac faecal occult blood tests (gFOBTs) or faecal immunochemical tests (FITs) (14). A full blood count is ordered in suspected CRC patients since iron deficiency, with or without anaemia, is the most common haematological finding in CRC.
Colonoscopy and biopsy
Colonoscopy assesses tumour location and allows simultaneous sampling of biopsy and histological evaluation, which is the gold standard for diagnosing CRC (8). The two predominant premalignant CRC lesions include serrated lesions and conventional adenomas (41). The quality of colonoscopy imaging has improved substantially during the last 20 years with the use of high-definition white light endoscopy (hWLE), which encompasses high-resolution video screens (8). Procedural risks associated to sedation, contraindication of administering bowel preparation due to the impeding risk of obstruction, operator dependency and its invasive nature may have contributed towards the alarming increase in CRC incidence within young adults (42).
CT colonography
CT colonography provides equal sensitivity as colonoscopy without the need for sedation, thereby allowing an endoluminal colon view using low-dose CT scanning. Therefore, it can be used as an alternative method of colonic assessment in patients who are unsuitable candidates or for whom colonoscopy is contraindicated. In comparison to double-contrast barium enema, CT colonography is the test of choice since it is better tolerated and more effective (41). However, radiation exposure and costs are important factors for consideration.
Flexible sigmoidoscopy
Flexible sigmoidoscopy allows visualization of the rectum and sigmoid colon and is highly sensitive in diagnosing left-sided CRC neoplasms at low cost and with minimal patient discomfort (23). Its major drawback includes a reduced benefit in protecting against right-sided CRC (41).
CT scan
Once a CRC diagnosis is made, a CT scan of the chest, pelvis and abdomen is essential for preoperative staging using oral and intravenous contrast, as well as for the identification of distant metastases (43).
Staging
CRC is classified using the tumour-node-metastasis (TNM) classification for staging. T describes the extent of tumour invasion depth in the various intestinal wall layers, N describes the number of lymph node involvement, and M describes the presence of distant metastasis. Stage I is limited to the intestinal wall and is early-stage cancer without metastasis to the lymph nodes; stage II is cancer without metastasis to the lymph nodes; stage III is cancer with lymph node metastasis but no distant metastasis and stage IV is cancer with presence of distant metastasis (24).
6. Pathophysiology
CRC can either occur sporadically (94%), or due to inherited mutations (5%) or may be derived due to chronic inflammatory bowel diseases (IBD) including Ulcerative Colitis or Crohn's disease (1%) (9).
Sporadic mutations and pathways of carcinogenesis
Sporadic mutations are associated with three proposed carcinogenetic pathways which include the chromosomal instability (CIN), the CpG island methylator phenotype (CIMP) and the microsatellite instability (MSI) pathways (23).
The CIN pathway
The CIN pathway is the most frequent mutated pathway in colon cancer corresponding to about 70% loCRC cases and 85% of eoCRC cases. It is characterised by an imbalance in chromosome number (aneuploidy) and loss of heterozygosity (22). In this pathway, the adenomatous polyposis coli (APC) gene, implicated in the WNT/β-catenin signalling pathway, underdoes loss-of-function mutations, which trigger abnormal crypt foci formation. Subsequently, inactivating mutations in tumour suppressor genes TP53 and activating mutations in proto-oncogenes KRAS and C-MYC can lead to the transformation of tubular adenomas into adenocarcinomas. Defects in this pathway are responsible for 85% of eoCRCs, which are associated with an increased rate of advanced histologic presentation, diagnosis at a later stage, and a reduced prevalence of CRC in the right colon (20,44).
There are differences in the genetic mutations reported in loCRC compared to eoCRC. In early onset CIN tumours, the loss of s chromosomal loci harbouring genes of the FOX transcription factor family as well as the TJP2 gene, can disrupt the regulatory control of gene expression, thereby contributing to carcinogenesis (45). The FOX transcription factor family comprises of numerous members and each member has a distinct roles in the regulation of various signalling pathways (e.g. the WNT/β-catenin pathway) (46). The TJP2 gene codes for the Tight Junction Protein 2 and plays a crucial role in the formation and maintenance of tight junctions (47). In CRC, TJP2 is mutated contributing to disrupted tight junctions and increased permeability, and potentially promoting carcinogenesis by allowing the escape of cancerous cells into surrounding tissues (48).
At the same time, early onset CIN tumours gain chromosomal loci which contain genes for BMPR1A (Bone Morphogenetic Protein Receptor Type 1A) and AMPK-(AMP-activated protein kinase) (45). The BMPR1A is gene associated with the BMP signalling pathway which plays a role in cell growth and differentiation. Mutations in the BMPR1A gene are linked to the Juvenile Polyposis Syndrome, a rare autosomal dominant condition characterized by multiple gastrointestinal hamartomatous polyps with a high risk of developing CRC (49). The regulatory subunit of AMPK is indirectly associated with CRC. Dysregulation of AMPK including its regulatory submit, can impact cellular energy metabolism and signalling pathways, contributing to carcinogenesis in the colon (50).
Contrastingly, late-onset CIN tumours lose chromosomal loci which contain the SMAD4, DCC and APC genes. The SMAD4 gene is considered a tumour suppressor gene since it encodes a protein that plays acritical role in the TGF-β signalling pathway regulating cell growth and apoptosis (45). The DCC (Deleted in Colorectal Cancer) gene is also considered as a tumour suppressor gene and encodes a receptor for the netrin-1 protein and functions in axon guidance during neural development (51). The APC (Adenomatous Polyposis Coli) gene regulates the Wnt signalling pathway and it is also a critical tumour suppressor gene; mutations in this gene are associated with the development of CRC through the promotion of uncontrolled cell grown and the formation of precancerous polyps (45).
The KRAS gene encodes a GTPase that participates in cell signalling pathways controlling cell growth and differentiation. KRAS can be considered an oncogene when it undergoes specific activating mutations that promote uncontrolled cell growth and contribute to cancer development. Mutations in KRAS are commonly found in CRC. A higher prevalence of mutations in the KRAS gene have been found among eoCRC (54%) in comparison to loCRC (40%) (52). The higher frequency of KRAS mutations in young individuals compared to older individuals suggest that these mutations are important in the development of eoCRC (45).
LINE-1 (Long Interspersed Nuclear Element-1), is a type of retrotransposon, a repetitive DNA sequence that can replicate and insert copies of itself at various locations in the genome (53).
LINE-1 hypomethylation is an epigenetic alteration i.e., a reduction in the methylation of LINE-1 retrotransposons in the DNA that is associated with genomic instability and may contribute to CRC by increasing the potential of genetic mutations and therefore activation of certain proto-oncogenes.
LINE-1 hypomethylation is an early CRC associated event; consistently lower levels of LINE-1 hypomethylation are found in eoCRC compared to loCRC. Moreover, associations between f LINE-1 hypomethylation with distal tumours and worse prognosis have been reported. LINE-1 hypomethylation is recognized as an independent factor for higher mortality, yet it is unclear whether this is a distinct feature of sporadic eoCRC (54).
The CIMP pathway
The CIMP pathway, corresponding to 30% of the sporadic CRC cases, involves hypermethylation of CpG islands contributing to the silencing of genes. Consequently, the promoter associated CpG-rich regions of tumour suppressor genes undergo inactivation of transcription leading to cancer development. In eoCRC, there is a lower number of BRAF mutations and reduced MLH1 promoter hypermethylation, compared to patients with later onset (55). Typically, CpG island methylation in colonocytes is an age-related phenomenon, and in young adults with CRC, this pathway is not usually observed since they undergo less extensive CpG island methylation (23).
The MSI pathway
The MSI pathway, accounting for 10-15% of the sporadic CRC cases, involves the disruption of DNA mismatch repair (MMR) genes that are normally responsible for identifying and repairing replication errors and proofreading newly synthesized DNA. This pathway is characterized by accumulation of single nucleotide mutations and modifications in the lengths of repetitive microsatellite nucleotide sequences. Tumours of this pathway occur in two forms of CRC: sporadic cases, where it involves epigenetic silencing (hypermethylation) of the MLH1 promoter, and hereditary cases like Lynch syndrome, which include germline mutations in the MMR gene (56). In comparison to CRC in older patients, where nearly all MSI cases represent sporadic MSI tumours, MSI in eoCRC is associated with germinal defects in all MMR genes (MLH1, MSH2, MSH6, PMS2) thereby causing various genetic predisposition syndromes (57).
The carcinogenic pathways are not mutually exclusive and can sometimes coexist The Microsatellite and Chromosome Stable (MACS) pathway can exhibit both chromosomal and microsatellite stability. Banerjea et al reported that the MACS pathway is most frequently reported in eoCRC patients with MACS tumours had lower survival than patients with CIN or MSI tumours (58). The MACS pathway is rarely associated with BRAF mutations, and presents with a different hypomethylation pattern than MSI and CIN (56).
Genetic predisposition syndromes
The two most common genetic predisposition syndromes for CRC include the Familial Adenomatous Polyposis (FAP) syndrome and the Hereditary Nonpolyposis CRC (Lynch syndrome). FAP arises mostly from the CIN pathway and prompts the formation of hundreds to thousands of adenomatous polyps during the individuals' adolescence. If left untreated, these individuals will subsequently develop CRC at approximately 40 years of age. Lynch syndrome emerges from the MSI pathway via inherited MMR gene mutations (56). There is an increased risk for CRC among young adults at an average age of 44 because of greater undiagnosed Lynch syndrome patients. Furthermore, there is a high risk of Lynch Syndrome patients developing extracolonic metastasis including endometrial, small intestine and ovarian metastasis (59).
Clinical trials
Ongoing clinical trials aim to identify different mutations occurring in eoCRC and to determine the significance of these in predicting the treatment outcomes.
One clinical trial (‘Genetic study of young patients with colorectal cancer’ (NCT00044967)) was conducted to determine the significance of gene mutations in helping predict the outcome of treatment in patients who develop stage I, stage II, or stage III CRC at an early age. The study was completed in 2004 but no results were posted (60). Furthermore, another clinical trial (‘Targeted Next-generation Sequencing Panel for Identification of Germline Mutations in Early Onset Cancers with Sporadic or Hereditary Presentation (PANEL)’ NCT02664389)), involved the sequencing of 200 selected somatic cancer genes of eoCRC patients, without genomic alterations in APC, MLH1, MSH2 and various other genes and was conducted to identify germline deleterious mutations. The study was completed in 2017 but no results have been published yet (61).
Lastly, another clinical trial (‘Young-Onset Colorectal Cancer’ (NCT02863107)) is being conducted to investigate the genetic factors that may contribute towards the development of CRC at a young age. Defining the clinical phenotype of young-onset vs. later onset CRC and examining germline genetic alterations in individuals with CRC and families at high risk of cancer may help identify new cancer genes. The study will be completed in 2030(62).
Differences in the histology of young vs. older CRC patients
Evidence in the literature supports that CRC in young adults more commonly occurs in the distal colon and rectum while older patients more commonly present with proximal tumours. The histological features which are distinct in young patients with CRC include a more aggressive pattern like signet-ring cell and mucinous tumours, in addition to poor differentiation. Furthermore, invasion of veins and perineuronal regions is more commonly observed in younger compared to older individuals (59).
7. Prevention
Primary prevention
Primary prevention is designed to prevent a disease or condition, from occurring and is targeting people not affected by the disease. Primary prevention includes the measures that prevent illness onset before the disease process begins. CRC focuses on encouraging lifestyle modifications including a healthy diet and increased physical activity which in combination can prevent obesity, and smoking cessation (63). Evidence from research studies supports that a higher consumption of dietary fibre or whole grains, calcium, and dairy and decreased consumption of red and processed meat and alcohol are associated with reduced CRC risk (6,64,65).
Health promotion targeting younger populations can ultimately help shape future lifestyle habits and enhance cancer prevention behaviours (44). A number of different strategies have been implemented with the scope of preventing eoCRC. One approach to effectively reach the target audience among 30-49 years of age is social media platforms, since in a national survey 98% of American adults from this age group have internet access (66). Organizations established by the government such as National Cancer Institute have used social media marketing strategies through multiple platforms and channels, such as blogs and Facebook to deliver a wide range of health promotion content (67). In countries with low socio-economic status like Ethiopia, CRC awareness is low (42,40%) and more than a third of the participants from a cross-sectional study evaluating CRC awareness in Ethiopia revealed that they received information related to CRC from mass media followed by social media. Participants who received information through social media were 2.5 times more likely to have high awareness of CRC than those getting information from other sources (68). Further evidence in the literature supports that health promotional campaign launches and access to peer support groups provide useful means to reach health consumers since these platforms help with provision of interactions, delivery of tailored material and enhanced access to health information (69).
In people with Lynch Syndrome, daily aspirin for longer than 2 years is recommended to prevent CRC (70). In addition, ongoing research is conducted to investigate whether primary prevention with aspirin in average/increased risk patients can reduce the risk of developing CRC (71). Low-dose aspirin is also recommended in adults 50 to 59 years of age with CRC who have a cardiovascular disease risk in the following 10 years and are not at risk of haemorrhage (72). Use of NSAIDs (except aspirin) was found to decrease the risk for CRC in patients 40 years and above with considerable effects mostly at higher doses, in women, white individuals and cancer at the distal colon (73).
Secondary prevention
Secondary prevention aims to minimize the impact of a disease that has already occurred and includes measures leading to early diagnosis and prompt disease treatment to halt or slow down its progress. Unlike other cancers, CRC is a slowly progressive cancer. Therefore, as a form of secondary prevention, adenomas can be detected and removed during colonoscopy. Early detection allows diagnosis at an earlier treatable stage and improves survival (63).
Successful CRC secondary prevention entails screening (72). Since the beginning of this century both the incidence and mortality of CRC for older individuals above 50 have decreased by about one-third due to screening colonoscopy (3). In contrast, the incidence and mortality in young adults who do not undergo screening are rising. For this reason, the American Cancer Society has decreased recommended age for commencing screening for CRC in the population from age 50 to 45(74). In 2021, the National Health Service (NHS) in England reduced the screening age from 60 to 50 years old, while the screening recommendations by the US Preventive Services Task Force start at 45 and continue through to 75 years old (75). Screening using colonoscopy from ages 45 to 75, instead of 50 to 75, has shown an estimated 6% increase in years of life gained, with a 17% increase in the number of colonoscopies performed (76).
First degree relatives of CRC individuals with documented advanced adenomas are instructed to begin screening on average 10 years before the youngest age that an affected first-degree relative was diagnosed or from the age of 40(41). The UK National Screening Committee recommends screening every 2 years from the age of 50 using FIT which has shown effectiveness in prevention and decreased mortality. It remains to be elucidated whether a combination of FIT screening and bowel scope testing provides additional benefit compared to FIT screening alone (77).
Strategies to enhance CRC screening compliance in eoCRC patients
Primary care providers play a key role in the prevention of CRC and have a major impact on the patients' compliance to successful screening (78). A successful increase in screening rates relies on implementing effective systems of decision support, such as electronic medical record reminders, as well as practices for screening delivery, like registries in the practices of primary care providers (79). Additionally, targeting high-risk patients by informing them about the significance and availability of routine screening tests could prevent delays in diagnosing cancer early, thereby improving patients' survival (80). FIT-based screening could achieve higher compliance rates when offered as part of organized screening programs, which include personal invitation letters with test kits and reminder letters (81).
In a systematic review of mailed FITs, potent interventions for improved screening comprised of telephone reminders with instructions, primary care provider encouragement, simplified kit tests, and letter notifications of incoming mailed tests sent in advance (82). In one study, a targeted mobile app was introduced among women aged 44-70 with the aim of enhancing CRC screening and providing each individual woman with the screening option best suited for her, based on her responses to the questions from the mobile app. The results from this study indicated the willingness of younger women under 50 to learn about their screening options and make informed decisions regarding CRC screening (83).
Future prospects look into using genome-wide association study results of polygenetic risk scores to determine risk categorisation (84). For individuals with Lynch syndrome, screening colonoscopy is usually recommended from the age of 20 to 25 years, while screening commences at the age of 10-12 years for individuals diagnosed with FAP syndrome (85). Guidelines from the British Society of Gastroenterology/Association of Coloproctology of Great Britain and Ireland (BSG/ACPGBI) recommend that people with Lynch Syndrome who carry mutations in the MLH1 and MSH2 gene should undergo colonoscopy from the age of 25 years of age whereas MSH6 and PMS2 gene carriers should undergo colonoscopy at the age of 35(86). The American Society for Gastrointestinal Endoscopy (ASGE) recommends that testing should begin at the age of 18 to 20 years if FAP is suspected (87).
Public Health England has launched invitation leaflets explaining CRC screening and colonoscopy to the public, which are available at screening hubs. Enhancing care and support in dealing with the effects of CRC and its treatment is the primary goal of the ‘Never Too Young campaign’, launched after the increase in CRC incidence in young individuals (88). The Colorectal Cancer Alliance in the USA uses survey reports from the Never Too Young Task force to track and learn about the self-reported medical, psychosocial and quality of life experiences of the young groups and address their needs and concerns (89).
Tertiary prevention
Tertiary prevention includes efforts to prevent the of complications in people who have already developed the disease and in whom disease prevention is no longer possible.
Several lifestyle factors are associated with improved clinical outcomes in cancer patients. Notably, one study has reported that incorporating physical activity into the lives of patients with stage III CRC who are actively receiving active chemotherapy is correlated with prolonged survival and improved prognosis (90).
The use of low-dose aspirin has also been observed to enhance the survival of patients following a CRC diagnosis emerging as a potential tertiary prevention strategy (91). Moreover, high-dose of vitamin D supplements have shown promise in improving progression-free life span in people with metastatic CRC, and as such, there are opportunities for further exploration of vitamin D in tertiary prevention (92). The American Society of Clinical Oncology has initiated efforts to enhance education, supporting people in understanding the pathophysiology of weight gain and introduce efficacious dietary habits in cancer survivors to help reduce obesity which is strongly correlated with CRC (93).
8. Conclusions
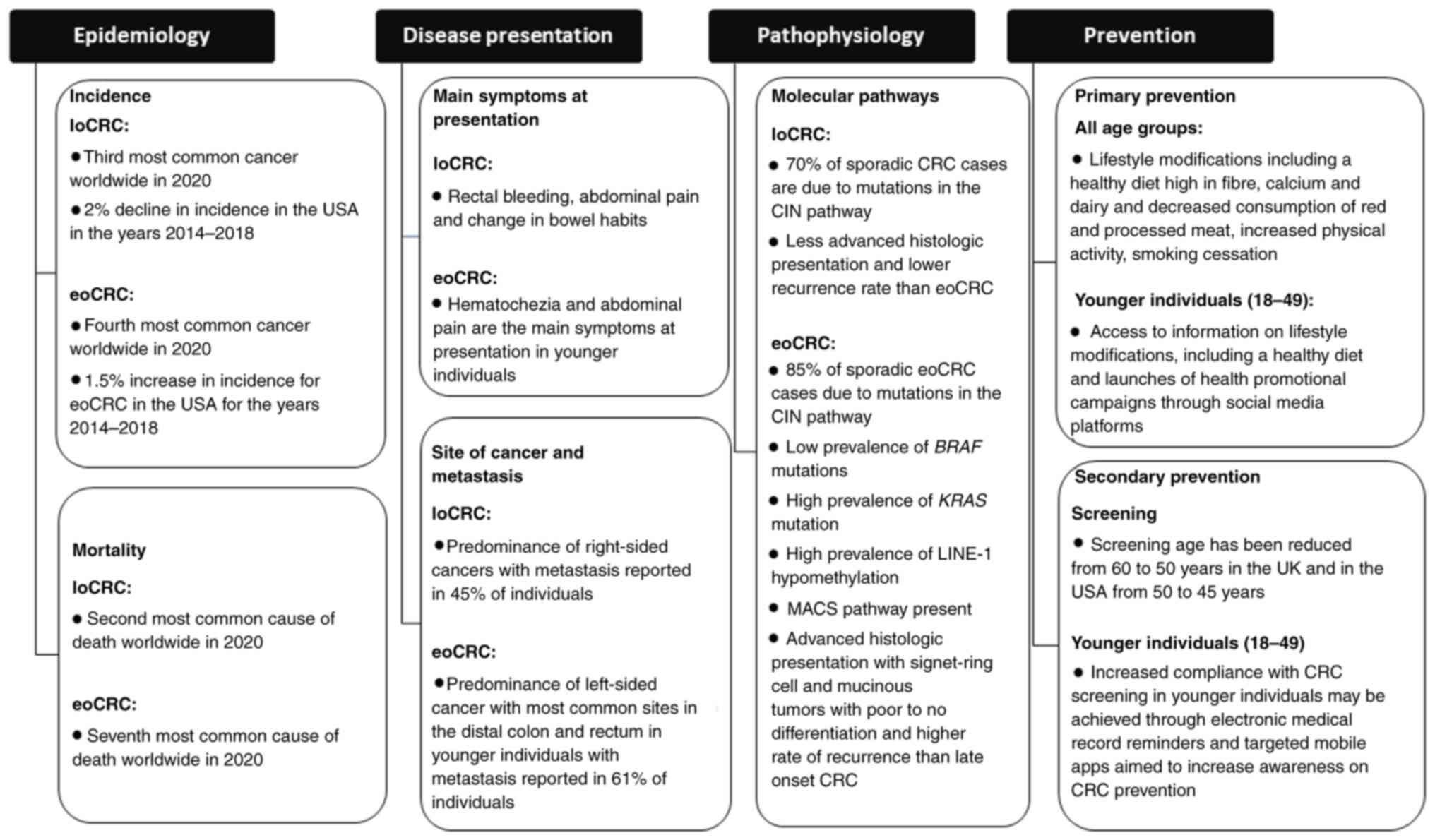
CRC presents a significant public health challenge, and it is expected that the incidence among young adults under the age of 50 will continue to rise in the following years. eoCRC differs from CRC in terms of epidemiology, disease presentation, pathophysiology, and prevention (Fig. 1). Analysing emerging trends in incidence and mortality, as well as identifying of risk factors (environmental, genetic, and behavioural) associated with CRC across different age groups, are promising future directions for the field. Genetic screening and counselling are particularly important due to the common genetic predisposition associated with CRC. Improving the information provided by primary care providers and using electronic medical record reminders, targeted mobile apps and simplified kit tests can enhance compliance and screening.
In the past few years there has been an increasing interest in eoCRC (94). Our narrative review builds on this interest and includes detailed epidemiological data on age-standardized incidence, prevalence, mortality, and survival in a wider range of countries with clearer trends in both loCRC and eoCRC. Different types of diagnostic tools are being discussed highlighting the advantages and disadvantages of each with regards to effectiveness, invasiveness, and sensitivity. The review also provides a brief overview of the importance of doctors obtaining a good family history from patients. In terms of prevention strategies, it includes a more thorough overview of the different levels of prevention and the various efforts used to raise awareness, strategies to enhance screening compliance as well as lifestyle changes. In addition, some clinical trials are included in order to show that indeed there are different carcinogenetic pathways involved in eoCRC and that different mutations are involved and may play a role in the clinical phenotype.
Currently, there is a pressing necessity to understand the most significant pathophysiological differences between eoCRC and lo CRC. In the near future, the use of multigene panels is expected to help identify the full spectrum of germline mutations and distinct molecular pathways in eoCRC patients compared to CRC in older patients. Furthermore, prospective cohort studies that will involve the collection of biospecimens from stool, saliva, and blood can be used to analyse the tumour microenvironment and metagenomics to help establish the aetiologies of eoCRC. The results of such studies will inform the design of randomized clinical trials with new drugs targeting mutations specific to eoCRC patients, providing insight into whether young patients can benefit from more specific treatment options based on new molecular targets.
In summary, establishing comprehensive and early risk assessment, targeted screening tools and improved molecular targets will have a significant impact on reducing the burden of eoCRC.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
VC and CC were involved in the conceptualization of the current manuscript, and in the literature search and review of the resources that were used in the current manuscript. Both authors were involved in the writing and revision of the manuscript, and read and approved the final manuscript. Data authentication is not applicable.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Authors' information
Dr Constantina Constantinou: ORCID iD: 0000-0001-6167-4023.
References
|
Xi Y and Xu P: Global colorectal cancer burden in 2020 and projections to 2040. Transl Oncol. 14(101174)2021.PubMed/NCBI View Article : Google Scholar | |
|
Siegel RL, Miller KD, Fuchs HE and Jemal A: Cancer Statistics, 2021. CA Cancer J Clin. 71:7–33. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Siegel RL, Torre LA, Soerjomataram I, Hayes RB, Bray F, Weber TK and Jemal A: Global patterns and trends in colorectal cancer incidence in young adults. Gut. 68:2179–2185. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Siegel RL, Miller KD and Jemal A: Cancer statistics, 2020. CA Cancer J Clin. 70:7–30. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Murphy CC, Sandler RS, Sanoff HK, Yang YC, Lund JL and Baron JA: Decrease in incidence of colorectal cancer among individuals 50 years or older after recommendations for population-based screening. Clin Gastroenterol Hepatol. 15:903–909.e6. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Stoffel EM and Murphy CC: Epidemiology and mechanisms of the increasing incidence of colon and rectal cancers in young adults. Gastroenterology. 158:341–353. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Zeki SS, Graham TA and Wright NA: Stem cells and their implications for colorectal cancer. Nat Rev Gastroenterol Hepatol. 8:90–100. 2011.PubMed/NCBI View Article : Google Scholar | |
|
Kuipers EJ, Grady WM, Lieberman D, Seufferlein T, Sung JJ, Boelens PG, van de Velde CJ and Watanabe T: Colorectal cancer. Nat Rev Dis Primers. 1(15065)2015.PubMed/NCBI View Article : Google Scholar | |
|
Fearon ER: Molecular genetics of colorectal cancer. Annu Rev Pathol. 6:479–507. 2011.PubMed/NCBI View Article : Google Scholar | |
|
American Cancer Society. Colorectal cancer facts and figures, 2020-2022. 2022. | |
|
Glover M, Mansoor E, Panhwar M, Parasa S and Cooper GS: Epidemiology of colorectal cancer in average risk adults 20-39 years of age: A population-based national study. Dig Dis Sci. 64:3602–3609. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Willauer AN, Liu Y, Pereira AAL, Lam M, Morris JS, Raghav KPS, Morris VK, Menter D, Broaddus R, Meric-Bernstam F, et al: Clinical and molecular characterization of early-onset colorectal cancer. Cancer. 125:2002–2010. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Fu J, Yang J, Tan Y, Jiang M, Wen F, Huang Y, Chen H, Yi C, Zheng S and Yuan Y: Young patients (≤35 years old) with colorectal cancer have worse outcomes due to more advanced disease: A 30-year retrospective review. Medicine (Baltimore). 93(e135)2014.PubMed/NCBI View Article : Google Scholar | |
|
AlZaabi A, AlHarrasi A, AlMusalami A, AlMahyijari N, Al Hinai K, ALAdawi H and Al-Shamsi HO: Early onset colorectal cancer: Challenges across the cancer care continuum. Ann Med Surg (Lond). 82(104453)2022.PubMed/NCBI View Article : Google Scholar | |
|
Chen FW, Sundaram V, Chew TA and Ladabaum U: Advanced-Stage colorectal cancer in persons younger than 50 years not associated with longer duration of symptoms or time to diagnosis. Clin Gastroenterol Hepatol. 15:728–737.e3. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Cercek A, Chatila WK, Yaeger R, Walch H, Fernandes GDS, Krishnan A, Palmaira L, Maio A, Kemel Y, Srinivasan P, et al: A comprehensive comparison of early-onset and average-onset colorectal cancers. J Natl Cancer Inst. 113:1683–1692. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Scott EC, Gardner EJ, Masood A, Chuang NT, Vertino PM and Devine SE: A hot L1 retrotransposon evades somatic repression and initiates human colorectal cancer. Genome Res. 26:745–755. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Tiritilli A and Ko C: Patients with early-onset colorectal cancer have an increased risk of second primary malignancy. Dig Dis Sci. 67:1328–1336. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Murphy N, Moreno V, Hughes DJ, Vodicka L, Vodicka P, Aglago EK, Gunter MJ and Jenab M: Lifestyle and dietary environmental factors in colorectal cancer susceptibility. Mol Aspects Med. 69:2–9. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Venugopal A and Carethers JM: Epidemiology and biology of early onset colorectal cancer. EXCLI J. 21:162–182. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Stanich PP, Pelstring KR, Hampel H and Pearlman R: A high percentage of early-age onset colorectal cancer is potentially preventable. Gastroenterology. 160:1850–1852. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Patel SG and Ahnen DJ: Colorectal cancer in the young. Curr Gastroenterol Rep. 20(15)2018.PubMed/NCBI View Article : Google Scholar | |
|
Segev L, Kalady MF, Plesec T, Mor E, Schtrechman G, Nissan A and Church JM: The location of premalignant colorectal polyps under age 50: A further rationale for screening sigmoidoscopy. Int J Colorectal Dis. 35:529–535. 2020.PubMed/NCBI View Article : Google Scholar | |
|
World Health Organization. International Agency for Research on Cancer. | |
|
Gu WJ, Pei JP, Lyu J, Akimoto N, Haruki K, Ogino S and Zhang CD: The Burden of early-onset colorectal cancer and its risk factors from 1990 to 2019: A systematic analysis for the global burden of disease study 2019. Cancers (Basel). 14(3502)2022.PubMed/NCBI View Article : Google Scholar | |
|
Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A and Bray F: Global patterns and trends in colorectal cancer incidence and mortality. Gut. 66:683–691. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Siegel RL, Miller KD, Fuchs HE and Jemal A: Cancer statistics, 2022. CA Cancer J Clin. 72:7–33. 2022.PubMed/NCBI View Article : Google Scholar | |
|
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: management of immunotherapy-related toxicities. 2022. | |
|
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, Bonaventure A, Valkov M, Johnson CJ, Estève J, et al: Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 391:1023–1075. 2018.PubMed/NCBI View Article : Google Scholar | |
|
SEER: An Interactive Website for SEER Cancer Statistics. Surveillance Research Program. National Cancer Institute, 2023. | |
|
American Cancer Society. Cancer Facts & Figures 2023. American Cancer Society, Atlanta, GA, 2023. | |
|
Liu PH, Wu K, Ng K, Zauber AG, Nguyen LH, Song M, He X, Fuchs CS, Ogino S, Willett WC, et al: Association of obesity with risk of early-onset colorectal cancer among women. JAMA Oncol. 5:37–44. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Okita Y, Koi M, Takeda K, Ross R, Mukherjee B, Koeppe E, Stoffel EM, Galanko JA, McCoy AN, Keku TO, et al: Fusobacterium nucleatum infection correlates with two types of microsatellite alterations in colorectal cancer and triggers DNA damage. Gut Pathog. 12(46)2020.PubMed/NCBI View Article : Google Scholar | |
|
Cao Y, Wu K, Mehta R, Drew DA, Song M, Lochhead P, Nguyen LH, Izard J, Fuchs CS, Garrett WS, et al: Long-term use of antibiotics and risk of colorectal adenoma. Gut. 67:672–678. 2018.PubMed/NCBI View Article : Google Scholar | |
|
BMJ Best Practice. 2022, 2022. Available from: https://bestpractice.bmj.com/info/. | |
|
Rho YS, Gilabert M, Polom K, Aladashvili A, Kopeckova K, Megdanova V, Coleman N, Greally M, Marrelli D, Roviello F, et al: Comparing clinical characteristics and outcomes of young-onset and late-onset colorectal cancer: An International collaborative study. Clin Colorectal Cancer. 16:334–342. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Kalady MF and Heald B: Diagnostic approach to hereditary colorectal cancer syndromes. Clin Colon Rectal Surg. 28:205–214. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Kolligs FT: Diagnostics and epidemiology of colorectal cancer. Visc Med. 32:158–164. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Holtedahl K, Borgquist L, Donker GA, Buntinx F, Weller D, Campbell C, Månsson J, Hammersley V, Braaten T and Parajuli R: Symptoms and signs of colorectal cancer, with differences between proximal and distal colon cancer: A prospective cohort study of diagnostic accuracy in primary care. BMC Fam Pract. 22(148)2021.PubMed/NCBI View Article : Google Scholar | |
|
Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D and Robertson DJ: Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society task force on colorectal cancer. Am J Gastroenterol. 112:1016–1030. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Gupta N, Kupfer SS and Davis AM: Colorectal cancer screening. JAMA. 321:2022–2023. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Vogel JD, Felder SI, Bhama AR, Hawkins AT, Langenfeld SJ, Shaffer VO, Thorsen AJ, Weiser MR, Chang GJ, Lightner AL, et al: The American Society of Colon and Rectal surgeons clinical practice guidelines for the management of colon cancer. Dis Colon Rectum. 65:148–177. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Lassi ZS, Salam RA, Das JK, Wazny K and Bhutta ZA: An unfinished agenda on adolescent health: Opportunities for interventions. Semin Perinatol. 39:353–360. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Cavestro GM, Mannucci A, Zuppardo RA, Di Leo M, Stoffel E and Tonon G: Early onset sporadic colorectal cancer: Worrisome trends and oncogenic features. Dig Liver Dis. 50:521–532. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Laissue P: The forkhead-box family of transcription factors: Key molecular players in colorectal cancer pathogenesis. Mol Cancer. 18(5)2019.PubMed/NCBI View Article : Google Scholar | |
|
Kim YJ, Jung YD, Kim TO and Kim HS: Alu-related transcript of TJP2 gene as a marker for colorectal cancer. Gene. 524:268–274. 2013.PubMed/NCBI View Article : Google Scholar | |
|
Martin TA and Jiang WG: Loss of tight junction barrier function and its role in cancer metastasis. Biochim Biophys Acta. 1788:872–891. 2009.PubMed/NCBI View Article : Google Scholar | |
|
Rosner G, Petel-Galil Y, Laish I, Levi Z, Kariv R, Strul H, Gilad O and Gluck N: Adenomatous polyposis phenotype in BMPR1A and SMAD4 variant carriers. Clin Transl Gastroenterol. 13(e00527)2022.PubMed/NCBI View Article : Google Scholar | |
|
Li W, Saud SM, Young MR, Chen G and Hua B: Targeting AMPK for cancer prevention and treatment. Oncotarget. 6:7365–7378. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Duman-Scheel M: Deleted in colorectal cancer (DCC) Pathfinding: Axon guidance gene finally turned tumor suppressor. Curr Drug Targets. 13:1445–1453. 2012.PubMed/NCBI View Article : Google Scholar | |
|
Watson R, Liu TC and Ruzinova MB: High frequency of KRAS mutation in early onset colorectal adenocarcinoma: Implications for pathogenesis. Hum Pathol. 56:163–170. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Rodić N and Burns KH: Long interspersed element-1 (LINE-1): Passenger or driver in human neoplasms? PLoS Genet. 9(e1003402)2013.PubMed/NCBI View Article : Google Scholar | |
|
Antelo M, Balaguer F, Shia J, Shen Y, Hur K, Moreira L, Cuatrecasas M, Bujanda L, Giraldez MD, Takahashi M, et al: A high degree of LINE-1 hypomethylation is a unique feature of early-onset colorectal cancer. PLoS One. 7(e45357)2012.PubMed/NCBI View Article : Google Scholar | |
|
Perea J, Rueda D, Canal A, Rodríguez Y, Álvaro E, Osorio I, Alegre C, Rivera B, Martínez J, Benítez J and Urioste M: Age at onset should be a major criterion for subclassification of colorectal cancer. J Mol Diagn. 16:116–126. 2014.PubMed/NCBI View Article : Google Scholar | |
|
Silla IO, Rueda D, Rodríguez Y, García JL, de la Vigo C and Perea J: Early-onset colorectal cancer: A separate subset of colorectal cancer. World J Gastroenterol. 20:17288–17296. 2014.PubMed/NCBI View Article : Google Scholar | |
|
Khan SA, Morris M, Idrees K, Gimbel MI, Rosenberg S, Zeng Z, Li F, Gan G, Shia J, LaQuaglia MP and Paty PB: Colorectal cancer in the very young: A comparative study of tumor markers, pathology and survival in early onset and adult onset patients. J Pediatr Surg. 51:1812–1817. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Banerjea A, Hands RE, Powar MP, Bustin SA and Dorudi S: Microsatellite and chromosomal stable colorectal cancers demonstrate poor immunogenicity and early disease recurrence. Colorectal Dis. 11:601–608. 2009.PubMed/NCBI View Article : Google Scholar | |
|
Ballester V, Rashtak S and Boardman L: Clinical and molecular features of young-onset colorectal cancer. World J Gastroenterol. 22:1736–1744. 2016.PubMed/NCBI View Article : Google Scholar | |
|
ClinicalTrials Gov: ‘Genetic Study of Young Patients with Colorectal Cancer’. NCT00044967, 2004. | |
|
ClinicalTrials Gov: Targeted Next-generation Sequencing Panel for Identification of Germline Mutations in Early Onset Cancers With Sporadic or Hereditary Presentation (PANEL). NCT02664389, 2017. | |
|
ClinicalTrials Gov: Young-Onset Colorectal Cancer. NCT02863107, 2023. | |
|
Brenner H and Chen C: The colorectal cancer epidemic: Challenges and opportunities for primary, secondary and tertiary prevention. Br J Cancer. 119:785–792. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Nimptsch K and Wu K: Is timing important? the role of diet and lifestyle during early life on colorectal neoplasia. Curr Colorectal Cancer Rep. 14:1–11. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Mehta SS, Arroyave WD, Lunn RM, Park YM, Boyd WA and Sandler DP: A prospective analysis of red and processed meat consumption and risk of colorectal cancer in women. Cancer Epidemiol Biomarkers Prev. 29:141–150. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Pew Research Center: Internet, Science & Techonology. 2023. Available from: https://www.pewresearch.org/topic/internet-technology/. | |
|
Miller AS: The zombie apocalypse: The viral impact of social media marketing on health. Journal of Consumer Health on the Internet. 17:362–368. 2013. | |
|
Hamza A, Argaw Z and Gela D: Awareness of colorectal cancer and associated factors among adult patients in jimma, south-west ethiopia: An institution-based cross-sectional study. Cancer Control. 28(10732748211033550)2021.PubMed/NCBI View Article : Google Scholar | |
|
Dixon HG, Pratt IS, Scully ML, Miller JR, Patterson C, Hood R and Slevin TJ: Using a mass media campaign to raise women's awareness of the link between alcohol and cancer: Cross-sectional pre-intervention and post-intervention evaluation surveys. BMJ Open. 5(e006511)2015.PubMed/NCBI View Article : Google Scholar | |
|
National Institute for Health and Care Excellence. Colorectal cancer. 2022. | |
|
Guo LL, Li YT, Yao J, Wang LS, Chen WW, He KY, Xiao L and Tang SH: Dairy Consumption and risk of conventional and serrated precursors of colorectal cancer: A systematic review and meta-analysis of observational studies. J Oncol. 2021(9948814)2021.PubMed/NCBI View Article : Google Scholar | |
|
Bibbins-Domingo K: U.S. Preventive Services Task Force: Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. preventive services task force recommendation statement. Ann Intern Med. 164:836–845. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Tomić T, Domínguez-López S and Barrios-Rodríguez R: Non-aspirin non-steroidal anti-inflammatory drugs in prevention of colorectal cancer in people aged 40 or older: A systematic review and meta-analysis. Cancer Epidemiol. 58:52–62. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Wolf AMD, Fontham ETH, Church TR, Flowers CR, Guerra CE, LaMonte SJ, Etzioni R, McKenna MT, Oeffinger KC, Shih YT, et al: Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 68:250–281. 2018.PubMed/NCBI View Article : Google Scholar | |
|
US Preventive Services Task Force. Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, Davis EM, Donahue KE, Doubeni CA, Krist AH, et al: Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA. 325:1965–1977. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Peterse EFP, Meester RGS, Siegel RL, Chen JC, Dwyer A, Ahnen DJ, Smith RA, Zauber AG and Lansdorp-Vogelaar I: The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: Microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline. Cancer. 124:2964–2973. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Bowel cancer screening: programme overview. 2023. Available from: https://www.gov.uk/guidance/bowel-cancer-screening-programme-overview. | |
|
Triantafillidis JK, Vagianos C, Gikas A, Korontzi M and Papalois A: Screening for colorectal cancer: The role of the primary care physician. Eur J Gastroenterol Hepatol. 29:e1–e7. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Clouston K, Katz A, Martens PJ, Sisler J, Turner D, Lobchuk M, McClement S and Crow G: CIHR/CCMB Team in Primary Care Oncology (PCO-NET). Does access to a colorectal cancer screening website and/or a nurse-managed telephone help line provided to patients by their family physician increase fecal occult blood test uptake?: Results from a pragmatic cluster randomized controlled trial. BMC Cancer. 14(263)2014.PubMed/NCBI View Article : Google Scholar | |
|
Gonzalez SJ, de Rubb MCM and Levine RS: Primary and secondary prevention of colorectal cancer: An evidencebased review. Family Medicine and Community Health. 5:78–84. 2017. | |
|
van der Vlugt M, Grobbee EJ, Bossuyt PM, Bongers E, Spijker W, Kuipers EJ, Lansdorp-Vogelaar I, Essink-Bot ML, Spaander MC and Dekker E: Adherence to colorectal cancer screening: four rounds of faecal immunochemical test-based screening. Br J Cancer. 116:44–49. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Goodwin BC, Ireland MJ, March S, Myers L, Crawford-Williams F, Chambers SK, Aitken JF and Dunn J: Strategies for increasing participation in mail-out colorectal cancer screening programs: A systematic review and meta-analysis. Syst Rev. 8(257)2019.PubMed/NCBI View Article : Google Scholar | |
|
Brittain K, Kamp KJP and Salaysay Z: Colorectal cancer awareness for women via facebook: A pilot study. Gastroenterol Nurs. 41:14–18. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Weigl K, Thomsen H, Balavarca Y, Hellwege JN, Shrubsole MJ and Brenner H: Genetic risk score is associated with prevalence of advanced neoplasms in a colorectal cancer screening population. Gastroenterology. 155:88–98.e10. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Syngal S, Brand RE, Church JM, Giardiello FM, Hampel HL and Burt RW: American College of Gastroenterology. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 110:223–262; quiz 263. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Monahan KJ, Bradshaw N, Dolwani S, Desouza B, Dunlop MG, East JE, Ilyas M, Kaur A, Lalloo F, Latchford A, et al: Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut. 69:411–444. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Yang J, Gurudu SR, Koptiuch C, Agrawal D, Buxbaum JL, Abbas Fehmi SM, Fishman DS, Khashab MA, Jamil LH, Jue TL, et al: American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes. Gastrointest Endosc. 91:963–982.e2. 2020.PubMed/NCBI View Article : Google Scholar | |
|
BowelCancerUK. 2022. Available from: https://www.bowelcanceruk.org.uk/. | |
|
Colorectal Cancer Alliance. 2023. Available from: https://socialpresskit.com/colorectal-cancer-alliance. | |
|
Van Blarigan EL, Chan H, Van Loon K, Kenfield SA, Chan JM, Mitchell E, Zhang L, Paciorek A, Joseph G, Laffan A, et al: Self-monitoring and reminder text messages to increase physical activity in colorectal cancer survivors (Smart Pace): A pilot randomized controlled trial. BMC Cancer. 19(218)2019.PubMed/NCBI View Article : Google Scholar | |
|
Frouws MA, Reimers MS, Swets M, Bastiaannet E, Prinse B, van Eijk R, Lemmens VE, van Herk-Sukel MP, van Wezel T, Kuppen PJ, et al: The Influence of BRAF and KRAS mutation status on the association between aspirin use and survival after colon cancer diagnosis. PLoS One. 12(e0170775)2017.PubMed/NCBI View Article : Google Scholar | |
|
Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, Panaccione R, Ghosh S, Wu JCY, Chan FKL, et al: Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet. 390:2769–2778. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Ligibel JA, Alfano CM, Hershman DL, Merrill JK, Basen-Engquist K, Bloomgarden ZT, Demark-Wahnefried W, Dixon S, Hassink SG, Jakicic JM, et al: American Society of clinical oncology summit on addressing obesity through multidisciplinary provider collaboration: Key findings and recommendations for action. Obesity (Silver Spring). 25 (Suppl 2):S34–S39. 2017.PubMed/NCBI View Article : Google Scholar | |
|
Saraiva MR, Rosa I and Claro I: Early-onset colorectal cancer: A review of current knowledge. World J Gastroenterol. 29:1289–1303. 2023.PubMed/NCBI View Article : Google Scholar |









